Article Text

Abstract
Across the globe, the well-being of newborns is significantly influenced by the knowledge and practices of family members, yet global health policies and interventions primarily focus on strengthening health services to save newborn lives. Predominant approaches to promote newborn survival in non-western cultures across the Global South are based on a western, nuclear family model and ignore the roles of caregivers within wider family systems, whose attitudes and practices are determined by culturally prescribed strategies. In this paper, I review evidence of a neglected facet of newborn care, the role and influence of senior women or grandmothers.
Based on a family systems frame, I reviewed research from numerous settings in Africa, Asia and Latin America that provides insight into family roles related to newborn care, specifically of grandmothers. I identified primarily published studies which provide evidence of grandmothers’ role as culturally designated and influential newborn advisors to young mothers and direct caregivers. Research from all three continents reveals that grandmothers play similar core roles in newborn care while their culturally specific practices vary. This review supports two main conclusions. First, future newborn research should be conceptualised within a family systems framework that reflects the structure and dynamics of non-western collectivist cultures. Second, newborn interventions should aim not only to strengthen health services but also influential family caregivers, particularly grandmothers and the indigenous social support networks of which they are a part, in order to improve family-level newborn practices and save newborn lives.
- child health
- public health
- review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Interventions to promote newborn health and survival in the Global South primarily focus on young mothers based on a Eurocentric view of nuclear family structure.
Evidences from studies in numerous cultural contexts across Africa, Asia and Latin America reveal the significant role and influence of experienced older women, or grandmothers, on newborn care within multi-generational family systems.
Research reviewed from non-western collectivist cultures across the Global South suggests that grandmothers play similar core roles with newborns through advising and direct caregiving while their culturally specific practices vary greatly.
Future newborn policies and research should be grounded in a family systems frame that reflects the structure and dynamics of families in non-western collectivist cultures.
Grandmothers’ knowledge is sometimes out of date, but given their proximity, authority and commitment to newborn survival they should be explicitly involved in newborn interventions in order to optimise this abundant local resource for newborn health and survival.
Introduction
The first days and weeks of life are critical for all newborns, especially in low-resource contexts in the Global South. Approximately 75% of newborn deaths occur in the first week of life, 40% on the first day and the majority occur at home.1 The family environment in which newborns begin life is critical to their health and survival, however, global efforts to promote newborn survival focus primarily on strengthening health services while giving limited attention to reinforcing family caregivers’ roles and practices.
Despite increased investment to reduce neonatal mortality, reduction has been slow.2 Essential family-level practices have been identified, for example, thermal care, exclusive breast feeding and evacuation of newborns when danger signs appear, yet efforts to support family caregivers have been limited. All non-western cultures have strategies to promote newborn survival with advisory and caregiving roles conferred on different family members around new mothers.3
This paper presents: the rationale for conceptualising newborn care within family systems; and examples of research from numerous contexts in Africa, Asia and Latin America that provide evidence of the role and influence of senior women, or grandmothers, on newborn care.
My discussion of newborn care within family systems is framed by fundamental features of the structure and dynamics of non-western collectivist cultures that have received limited attention in global efforts to promote newborn survival.
Conceptual framework
Culture: a neglected parameter in global health
For many years, anthropologists have lamented the limited attention given to culture in global health.4 Airhihenbuwa articulates this concern in his seminal book, Health and Culture: Beyond the Western Paradigm arguing that health programmes in Africa have ‘consistently undermined, and in most cases ignored, the centrality of culture’ often resulting in culturally inappropriate interventions.5 (p. x) From an Asian perspective, Kumar et al discuss the primacy of the sociocultural context in community health and assert that many newborn interventions are culturally blind.3 Inadequate clarity on the notion of culture contributes to its neglect. Weidman delineates two fundamental dimensions of health culture: cognitive and normative health-related values and beliefs; and the social system, including roles, relationships and health-seeking patterns, in which health-related events occur.6 Most community health research and interventions primarily focus on the first dimension, involving individual-level psychological factors, while giving limited attention to the wider social context.7
Characteristics of collectivist cultures
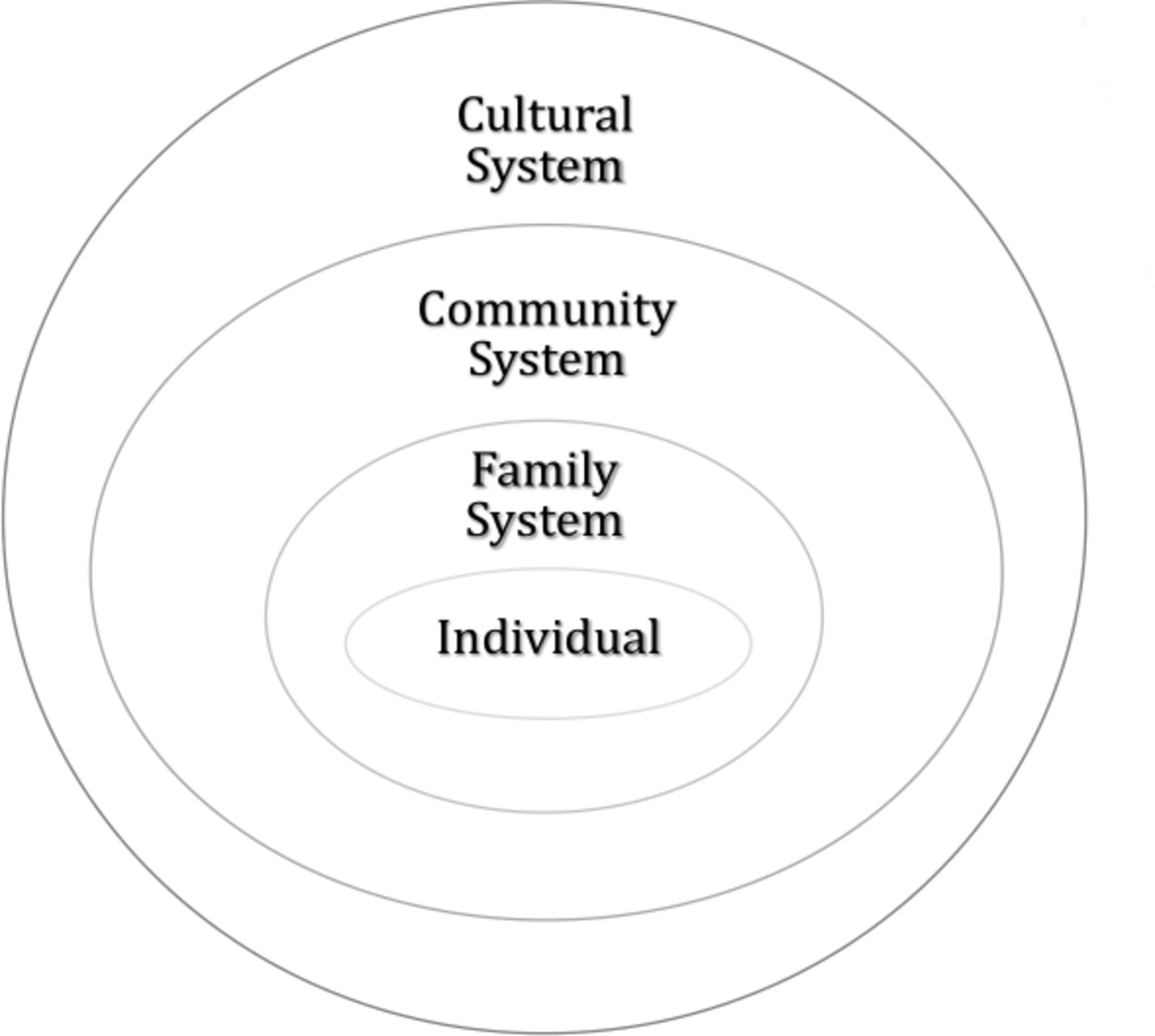
On a continuum from individualist to collectivist, approximately 88% of all societies are fundamentally collectivist.8 The collectivist structure of the Majority World should be a central consideration in newborn research and interventions. Salient characteristics of collectivist cultures that should orient newborn programmes include: hierarchy based on age and experience; elders are teachers of younger generations; gender-specific roles; multigenerational families and childrearing; collective decision making and interdependency valued over autonomy.9 The position of individuals in collectivist cultures, nested in family, community and cultural systems, is visualised in the onion model9 (figure 1).

{kind=link}
Onion Model. Individuals are embeddedin family, community and cultural systems. Aubel and Rychtarik.9
Asian researchers contrast the western ideal of individual agency with the non-western value of collective agency.10 Similarly, in the African concept of Ubuntu, individuals value interdependency over autonomy.11 And Turkish psychologist Kagitcibasi contrasts western cultures of separateness with eastern cultures of relatedness and interconnectedness.12 For example, for a young pregnant woman in Mali or Bangladesh, embedded in the onion, it is extremely difficult for her to reject the expectations of family, community and culture. She is expected to conform while concurrently she receives valuable support from those around her.
African anthropologists identify generally ignored facet of collectivist family values.13 They explain that in African cultures, a child belongs to, and is the responsibility of the extended family. Collective responsibility for raising children has clear implications for newborn research and interventions, however, it is consistently overlooked in global health frameworks and interventions which narrowly focus on biological parents and offspring.
Household production of health
Historically, community health interventions have primarily focused on formal health systems while neglecting family health systems.14 In the 1990s, a group of prominent social scientists asserted that determinants of child health emanate primarily from within households. They proposed the household production of health (HPH) framework asserting that child health interventions should build on intra-household roles, dynamics and decision making.15
HPH proponents emphasised the influence of culture on child health related to three aspects of non-western households: several categories of household actors participate in caregiving; roles of men and women are gender-specific and child health practices are culturally prescribed. The HPH framework implies a profound conceptual shift from a narrow focus on women and children to an inclusive family systems perspective.15 While the ground-breaking HPH work has been largely forgotten, current interest in socioecological or systems, approaches to addressing health issues echoes the perspective of the HPH pioneers.16
Reconsidering the mother–child dyad
A key focus of maternal and child health (MCH) policies, research and programmes is the mother–child dyad, rooted in the risk group orientation and nuclear family model. While this concept has been widely embraced in public health in the Global South, it is incompatible with the structure of non-western collectivist cultures where mothers and children are embedded in extended family systems. The misfit between the reductionist mother–child dyad frame and the influence of extended families in collectivist cultures is confirmed by research on household structure in 31 Sub-Saharan African countries. ‘Most mother–child dyads are not self-contained units but are part of a larger family system in which mothers are supported by other family members and in particular by grandmothers’.17 (p. 91)
A small, but growing, body of research on collectivist cultures in the Global South looks beyond the mother–child dyad and biological parents, elucidating the roles and influence of both kin and non-kin advisors and caregivers in MCH.18 This research on MCH topics offers increased insight into family systems structure and dynamics and consistently reveals the central role of senior women, or grandmothers, in rural contexts, for example, in India19 and Brazil20 and also in many urban settings for example, in Nairobi21 and Quito.22 (Buitron, Thesis, 2018) From a systemic view of families in collectivist Brazil, researchers propose recentring MCH’s focus on the child–mother–grandmother triad.23
Hierarchy based on gender and experience
Collectivist cultures are hierarchically structured, and authority is associated with gender, age and experience. Men’s and women’s roles are gender specific and with age and experience, their authority increases in their respective domains of responsibility. ‘Behaviours are passed on from older, more experienced actors to younger, lesser experienced actors’.3 (p. 455) In collectivist cultures, for all MCH matters, major responsibility lies with female family members whose knowledge and experience increase with age.18 Consequently, across non-western cultures, families recognise senior women as authorities on all aspects of child development, often advising men on the support they should provide. ‘In Southeast Asia, grandmothers are considered storehouses of knowledge and wisdom on a wide array of household topics’regarding MCH.24 (p.2115) Grandmothers’ influence often extends beyond the family. Research in 5 West African countries documents the role of influential networks of senior female kin and non-kin in newborn care collectively coaching and supervising women during pregnancy and postpartum.25
Limitations of newborn frameworks
Neonates are embedded in families where there are multiple caregivers. Unfortunately, global newborn policy frameworks give limited attention to the roles of various family caregivers. For example, one objective of the 2014 WHO/UNICEF Every Newborn Action Plan is to harness the power of parents, families and communities, however, no reference is made to intrafamilial roles beyond that of parents.26 UNICEF’s 2018 framework, Every Child Alive, prioritises improving health facility newborn care but makes no mention of the need to strengthen family caregiving.2 Factors that can explain this omission include: the medicalised focus on health services for newborns; the Eurocentric assumption that mothers are autonomous caregivers5; inadequate understanding of multi-generational caregiving in families; the deficit model in public health which ignores community assets27; and ageist biases, particularly against older women.
Evidence of grandmothers’ role in newborn care
In the second part of the paper, I review evidence of the role and influence of grandmothers on newborn care from published reports of qualitative research from Africa, Asia and Latin America, conducted since 2000, and published in English, Spanish and French. Studies reviewed were identified through periodic manual searches over the past 10 years in Google Scholar, Research Gate and PubMed using these key words: newborns; neonatal; MCH; and grandmother. I identified more than 70 studies from 29 countries, primarily in published articles but also in grey literature obtained mainly through personal contacts with international development organisations. Due to space limitations, I refer to only a selection of the 70 studies in the following discussion.
Analysis of the identified research focused on three components of family systems proposed by Aubel and Rychtarik: core cultural values related to women and children; family and community roles related to newborn care; and cultural norms and practices with newborns.9 Based on this family systems framework, research findings regarding seven themes related to family level newborn care are presented.
Grandmothers’ role as authoritative advisors and caregivers
An earlier review presented evidence of the role of senior women, collectively referred to here as grandmothers, as caregivers and advisors on child nutrition in the non-western world.18 Here, research from Africa, Asia and Latin America provides evidence of the dual-faceted role of grandmothers providing newborn care and advising young mothers, for example, from Africa: Ethiopia28; Ghana29–31; Kenya21; Benin13; Mauritania25; Malawi32; Niger33; Nigeria34; Egypt35; Burkina Faso36; Senegal37; Nigeria, Tanzania and Ethiopia.38 Mali39; and Uganda40; from Asia: India27 41–43; Pakistan44; Nepal24; Indonesia45; and from Latin America: Brazil46 ; Mexico(Ramos, thesis, 2014); Costa Rica47; Colombia.48
Research conducted in this wide array of sociocultural contexts reveals similar gender-specific and age-specific roles of family members in newborn care with consistent recognition of grandmothers’ expertise and authority. Brazilian researchers report that young urban mothers refer to grandmothers as their eternal guides, ‘They brought security and comfort justified by the experience accumulated by these women’23 (p.537) and breastfeeding research in urban Mexico concludes, ‘grandmothers continue to play a leadership role in families as primary advisors and health promoters’ (Ramos thesis, 2014, p.40). Two studies in Ghana conclude, ‘parents consider grandmothers as the epitome of wisdom and knowledge regarding newborn care’31 (p.5) and it is the husband’s mother who calls the shots on newborn care.29
In Nepal researchers concluded that advice from revered and authoritative grandmothers cannot be refused.24 Indian researchers report on grandmothers’ influence within the web of social relationships surrounding and influencing younger mothers.19 A similar pattern emerges across non-western cultural settings: newborn care is coordinated by older women; younger women are learners; and men are rarely directly involved.
Inculcating cultural norms and practices
As culturally designated authorities on newborn care, grandmothers are responsible for transmitting an array of culturally prescribed practices involving: massage; cord care; colostrum; prelacteals; thermal care; breast feeding; newborn illness and spiritual protection. While certain traditional practices conveyed by grandmothers are beneficial, others are not, such as giving prelacteals and withholding colostrum. In Karnataka, grandmothers initiate young mothers to the use of prelacteals, cord and thermal care.49 Egyptian grandmothers give newborns herbal drinks to stop babies from crying at night.35 In Nigeria grandmothers’ harmful practices include giving water, prelacteals and traditional medicines34 while in Brazil grandmothers give traditional teas and water to newborns.50 In Northern Ghana, grandmothers’ demonstrate ancestral traditions involving placenta burial and breastmilk stimulation.29 Across cultures, grandmothers’ training efforts are greater with primiparas, to instil practices that should be replicated with subsequent newborns, for example, in Uganda.40
Young mothers are expected to defer to the advice of their recognised senior advisors. Newborn research in four African sites documents young mothers’ dependency on experienced grandmothers where often ‘mothers themselves only took full responsibility of newborn care after a few days or weeks’.38(p.1262) Similarly, in Nepal young mothers cannot refuse directives on traditional newborn practices from revered grandmothers.24 Many studies, for example, in Malawi32 Mauritania25 and India19 document mothers’ adherence to grandmothers’ traditional advice on infant care, given their trust and respect for them, even when it conflicts with health workers’ advice.
Seclusion of mothers and newborns: protecting and teaching
In many cultural settings, initial newborn care, protection and feeding involve seclusion of infants and mothers, for varying lengths of time, usually under the supervision of an experienced grandmother or other senior female family member. In Karnataka, during 40 days of confinement49 and in Nepal during 6 days of chhatiyar, grandmothers transmit their experience concerning all aspects of newborn care and feeding, to new mothers.51 In Senegal, 7 days of seclusion protects newborns from the mystical we illness.37 Studies in many other cultural contexts describe this protective and educational period of isolation for babies and mothers, for example, in Indonesia,45 Niger,33 Burkina Faso,36 India3 and Amazonia.20
Grandmothers’ role in breast feeding
There is extensive evidence of grandmothers’ influence on whether and how long young mothers’ breastfeed. While mothers may receive occasional advice from health workers, most women benefit from in-house breastfeeding coaches, that is, grandmothers and other experienced female family members, for example, in Ghana,52 Benin,13 Mauritania25 and Brazil.50 In Bihar, mothers-in-law are primary decision-makers on breastfeeding initiation, practices and problems.42
In urban Ecuador, most new mothers identified grandmothers as their primary breastfeeding advisors and all others cited other older female kin and non-kin.(Buitron, Thesis, 2018) In urban Mexico,(Ramos, Thesis, 2014) grandmothers’ advice was the main determinant of whether young mothers breastfed. Based on social network analysis, other Mexican researchers found that most women (95%) were primarily encouraged to breastfeed by maternal grandmothers, while less encouragement came from doctors (58%) and from paternal grandmothers (42%).53
Some studies report on grandmothers’ advice for increasing breastmilk production, for example, from urban Bangladesh54 and rural Ghana.29 Grandmothers often advise certain foods and liquid drinks for lactating women, for example, in urban Bangladesh both kin and non-kin grandmothers advise specific foods to increase breastmilk.54
In many cultures, grandmothers believe that some breastmilk is of poor quality or insufficient quantity, for example, in Ghana55 and Egypt,35 ideas refuted by nutritionists. In Egypt, grandmothers believe that breastmilk is poor quality when a baby cries after breast feeding and this justifies giving herbal drinks to infants.35 As discussed above, while grandmothers’ advice may be erroneous, it is often very difficult for young mothers to reject the advice of their resident senior breast feeding advisors.
Care of sick newborns
Most research on newborn illness focuses on health services and technologies. Few studies have systematically investigated household-level strategies to care for sick neonates. Evidence from various non-western contexts reveals that during neonatal illnesses, families recognise grandmothers’ expertise to diagnose problems, to provide home treatment and to determine if extrafamilial support is necessary. In Ghana, researchers concluded that ‘Older women and grandmothers are often the ones who decide that a child is in need of treatment and often also determine the type of treatment due to their authority within the household and the community’”.30 (p.125) There are similar findings on grandmothers’ central role in caring for sick newborns from Mali,39 Indonesia45 and India.10 41 42 As in other contexts, in Nepal researchers found that decision making around newborn illness is a collective process mainly involving female family members, with husbands playing a limited role.51
In many societies, there are mystical newborn illnesses that medical doctors do not understand but that grandmothers have experience treating, for example, in India10 and Senegal.37 Across Latin America the folk illness, empacho, is treated outside the formal health system by grandmothers, aunts and female neighbours.56
Indigenous newborn support systems
In collectivist non-western cultures, solidarity and reciprocity are primordial values reflected in the spirit of cooperative breeding 57 and embodied in ubiquitous women-centred, multigenerational indigenous support systems for women and children.18 Unfortunately, the influence of these social support networks on pregnancy, newborn and child health has been largely unexplored in research in the Global South. South African, Steuart, was an early observer of these naturally occurring networks and referred to them as primary friendship groups.58 In Mali, researchers identified four types of support for MCH provided by these social networks: practical, informational, emotional and material or tangible assistance.59 In the extensive research on newborn research, these social networks has been largely ignored, reflecting the Eurocentric and reductionist focus on nuclear families and mother–child dyads.
A few studies have investigated the influence of these social networks, composed primarily of experienced older women, kin and non-kin, for example, in Nepal60 and Benin.13 Research in Odisha describes these indigenous social support networks as webs of social influence that are ‘powerful disseminators of knowledge’ to young mothers on newborn care.19 (p.113) A very significant finding from this research in India is that compared with better-educated women, less-educated women’s health knowledge is more influenced by their social networks, composed primarily of older women, than by formal health workers.19
In all contexts, these social networks convey to younger women not only prescribed practices but also provide them with crucial emotional support. Most studies that discuss grandmothers’ role in newborn care, focus on their knowledge and practices, while giving little attention to the emotional support they provide to young mothers. Costa Rican researchers discuss the importance to young mothers of grandmother social support networks, or redes de apoyo.47 From two different contexts in Brazil20 23 researchers describe the invaluable contribution of these networks in creating social bonds between women around newborn care which often provide ongoing reciprocity and support.
Men’s role in newborn care
Many current MCH programmes target fathers, however, there is a dearth of in-depth research on men’s roles in MCH within family systems in non-western contexts. Many studies from different sociocultural contexts conclude that: men do not play an active role either in direct caregiving nor in day-to-day decision-making concerning newborns; and that men play important supporting roles, particularly during newborn illnesses, providing logistical and financial help, for example, in Benin,13 Ghana,29 Burkina Faso,36 Mali,39 Niger,33 Senegal,37 Nepal51 and Indonesia.45 This same pattern regarding men’s involvement is reported from four African contexts supporting the conclusion that ‘physical and social spaces related to newborn care were closed to men, that men were perceived to lack the ability to care for the newborn and had little physical contact with the baby, but as head of the family, they were often the symbolic decision-makers and the financial provider’.38 (p.1263)
Families recognise that newborn care requires specialised expertise which men do not have. In many cultural settings during the first days after birth men are excluded from gendered newborn spaces.18 It is often erroneously assumed that men, as head of household, are primary decision-makers on all family issues. The research reviewed here supports the conclusion that for newborn care men are rarely central decision-makers and more often are advisees of experienced women within the family.
A present trend, reflecting nuclear family structure in the Global North, is the promotion of men’s involvement in all aspects of MCH, including newborn care, based on the assumption that greater men’s participation is always advantageous. Some researchers have questioned this assumption, expressing concern that increased men’s involvement and authority in the newborn space can inadvertently disempower women and disrupt the women-to-women support system for mothers and neonates. Research in multiple African settings supports the conclusion that “care must be taken to ensure that interventions to involve men do not result in disempowerment of female family members”.38 (p.1263)
Conclusions
This discussion on newborn care with families in Africa, Asia and Latin America provides insight into an aspect of newborn health that heretofore has been given limited attention—the role of grandmothers. A growing body of evidence from across non-western, collectivist societies reveals the culturally designated role of these experienced, older women as newborn advisors and caregivers. Unfortunately, at the global level, newborn research, policies and interventions continue to focus primarily on medical technologies and services,61 to a lesser extent on mothers while giving little attention to intrahousehold newborn strategies in which grandmothers are key components of families’ sociocultural operating systems.4
Research identified from 70 cultural contexts across Africa, Asia and Latin America reveals significant commonalities regarding core roles played by grandmothers with newborns, while their culture-specific practices can vary greatly. Grandmothers’ core roles are summarised by researchers in Ghana ‘Grandmothers play an integral and multifaceted role in maternal and infant health. Grandmothers support mothers during pregnancy, care for infants following delivery, maintain cultural traditions surrounding pregnancy and childbirth and serve as repositories of knowledge on local treatment options’.29 (p. 9) These core roles of Ghanaian grandmothers during pregnancy and with newborns are virtually the same as those of grandmothers identified in studies from all three continents.
Grandmothers’ central role in newborn care in non-western societies emanates from the structure and core values of collectivist cultures where: reciprocity and solidarity are key values; the social hierarchy in families is determined by gender and age; roles are gender-specific; social norms are transmitted from older to younger women; there is collective responsibility for children, especially among female caregivers; and decision-making is collective, with experienced elder women having authority. A vital social resource for MCH in collectivist cultures, that is very beneficial to newborns are the indigenous social support networks of women, both kin and non-kin, who collaborate to ensure optimal newborn care within families.18 These networks demonstrate what evolutionary anthropologists refer to as cooperative breeding where mothers, across the species, are supported by others, mainly female kin, and non-kin, in raising their offspring.57 61 62
Many studies report that grandmothers’ knowledge is not up to date and that some of their newborn practices are harmful, such as giving prelacteals. The research reviewed clearly reveals that while their knowledge is often inadequate, they wield significant influence over both younger mothers and other family members, based on the belief in and respect for their experience. Grandmothers’ authority and power is demonstrated by the fact that respectful daughters and daughters-in-law often hesitate to contest their senior advisors’ instructions when they differ from health workers’ advice.
This research reviewed represents a growing, but still minor, stream of research on grandmothers’ role in newborn care in the Global South. Hundreds of past studies on MCH issues in non-western cultures make no mention of grandmothers’ role. What can explain this oversight? In my analysis, this discrepancy points to inadequacies in the dominant conceptual frameworks used in research, of Euro-American origin, which fail to take into account the structure and dynamics of extended family systems in non-western, collectivist cultures.7 12
Most studies on newborn care in the non-western world are conceptually grounded in a western model of the nuclear family where: care for neonates is the responsibility of biological parents; the roles of women and men overlap; grandparents often are not nearby; and young parents give greater credence to doctors’ advice than to that of their elders. Conceptual frameworks for research across the non-western world, cloned from the West, consistently overlooks the distinct features of collectivist societies.12 Research on newborn caregiving, primarily investigates mothers’ knowledge and practices, and sometimes those of fathers, while giving limited attention to the wider family systems in which newborns are embedded.
Future research should investigate characteristics of family systems in collectivist cultures related to: gender-specific roles in families related to MCH; multigenerational involvement in childcare; the hierarchical structure of authority among women, related to age and experience; roles of men and women of different generations; collective decision making within families; roles of men and women of different generations; and men’s involvement in different facets of MCH.
Regarding men’s involvement in newborn care, my review of existing research presents a consistent finding that men are very rarely directly involved in newborn care. These findings question the frequently held assumption that men are central actors and decision-makers in all aspects of family life, perhaps overestimating the power of the patriarchy. The supposition regarding men’s hegemonic role in women’s and children’s lives in non-western families is questionable in two respects. First, evolutionary and biological anthropologists now question long-standing assumptions regarding males’ central role in child rearing in human societies in light of cooperative breeding patterns where females play a leading role.57 61 Second, several non-western female social scientists critique the historical discourse which places men at the centre of all family life.
Nigerian anthropologist, Amadiume, asserts that excessive attention has been given to the patriarchal paradigm, while at the centre of African families’ social life is a matriarchal system which has gone largely unrecognised.63 She vehemently questions widely held assumptions about the all-encompassing authority of the patriarchy in female domains of responsibility in family life and emphasises the importance of the matriarchy in those spaces.
Similarly, from a South Asian perspective on gender dynamics, Mumtaz critiques the overemphasis on men’s influence on women’s lives and calls attention to the importance of women-to-women bonds and intergenerational female relationships wherein younger women’s ties with experienced and wise older women are particularly edifying.64 These rarely heard critiques of the notion of men’s all-encompassing authority in the lives of women and children evoke the need for greater investigation into women-centred systems of collaboration and authority within family systems.
Several recent experiences using a grandmother-inclusive approach to address health issues related to grandmothers’ areas of responsibility and expertise provide evidence of their potential to contribute to positive health-related outcomes. Evaluations of these innovative programmes have shown positive results strengthening grandmothers’ knowledge, caregiving competencies and advice to other family members and increasing programme outcomes.
Encouraging results of grandmother-inclusive interventions are reported from: Nepal concerning antenatal and newborn care65; Uttar Pradesh addressing newborn care3; Malawi, dealing both with newborn care66 and adolescent HIV prevention67; Burkina Faso addressing child nutrition68 and Senegal addressing child nutrition69 and adolescent health issues.70 71 These several positive experiences, using a grandmother-inclusive approach in different cultural contexts, suggest that grandmothers may not be as intransigent to change as often assumed. These results also support the need for further experimentation with and evaluation of grandmother-inclusive interventions addressing newborn, other MCH and adolescent issues.
Two major recommendations emerge from this discussion supporting the need: to reconceptualise newborn research and interventions; and to involve grandmothers in newborn interventions.
First, existing evidence on the role and influence of grandmothers on newborn health highlights the incongruity between the decisive role played by these culturally designated newborn advisors and caregivers and the fact that most newborn policies and programmes virtually ignore their role in the lives of newborns and the enormous social resource they represent for community newborn interventions.
To more effectively promote newborn health and survival I contend that there is a need for a major conceptual shift in newborn research to overcome the prevailing conceptual bias which reflects a Eurocentric view of families rather than the structure and values of more collectivist non-western societies.7 16 Making this shift will require revision of prevailing conceptual frameworks and development of alternative research methodologies. This reframing should contribute to better understanding communities’ emic perspective and lead to more effective strategies to promote newborn survival. Pioneering work by some scholars from the Global South exhibits a more systemic and culturally grounded frame for MCH research on intra-household dynamics indicating their greater cognizance of both the structure of collectivist cultures and of the critical role played by elders within those systems.
Second, the numerous studies reviewed here provide extensive evidence of grandmothers’ role as caregivers and decision-makers in newborn care across the Global South. Extant research supports the assertion that the involvement of grandmothers in newborn care is beneficial to young mothers and to newborns, however, it is also reveals that some of grandmothers’ knowledge and practices are out of date, and sometimes harmful. Most studies strongly advocate for their inclusion in future newborn interventions based on their power and influence within their respective cultures and on the notion that their involvement may strengthen their knowledge and practices.
While all research reviewed provides evidence of grandmothers’ influence on newborn care, surprisingly, some does not explicitly recommend their inclusion in future programmes. Unfortunately, there is continued reluctance to explicitly involve grandmothers in interventions addressing newborn and other MCH issues. This appears to be related to: the often-repeated idea that grandmothers are barriers to change; a narrow perception of grandmothers focusing on their harmful traditional practices; and gender and ageist biases toward older women.
Policy and programme planners should realise that the failure to explicitly include these cultural authorities can be perceived by grandmothers themselves and by their communities as an affront to their culture and engender resistance to well-intentioned programmes, thereby limiting their effectiveness. This review provides support for the use of unconventional, but culturally grounded criteria for choosing community target groups for newborn interventions, namely, cultural authority, age and experience with newborns.
Acknowledgments
Gratitude is expressed to Dr Tina Grybowski and Alyssa Rychtarick for their help in identifying the literature reviewed here and for their inputs into earlier drafts of the paper.
References
Supplementary materials
Footnotes
Handling editor Stephanie M Topp
Contributors JA conceptualised the research, analysed the studies reviewed, interpreted the data, wrote and revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement This paper no data is referred to.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.