
In June 2021, American physician Peter McCollough spoke to faculty and students at IHU Méditerranée in Marseille, France. Dr. McCollough has been a vocal critic of the way the coronavirus pandemic has been handled in his country. With his colleagues, he developed a successful treatment protocol, after which he has protested strongly against the suppression of information about this treatment. He has also been critical of the way vaccination programs in the United States have been deployed hastily without the extensive and objective safety surveillance that vaccination programs are normally subjected to. His presentation can be seen at the link below, while excerpts of it follow in this post.
This post also includes short excerpts from two other talks at IHU Méditerranée in early July 2021. One of them was given in English, and the other in French, so the first excerpt is a transcript and the second is a translation.
“Early ambulatory therapy with a sequenced multi-drug regimen is supported by available sources of evidence and has a positive benefit-to-risk profile. We just need to look for signals of benefit and acceptable safety. We’ve shown we can reduce hospitalization and death. We can more safely buy time until we can get to a safe vaccine. The Covid 19 genetic vaccines’ unfavorable safety profile cannot be generally supported in clinical practice at this time.”
TRANSCRIPT EXCERPTS
The Successful Treatment Protocol
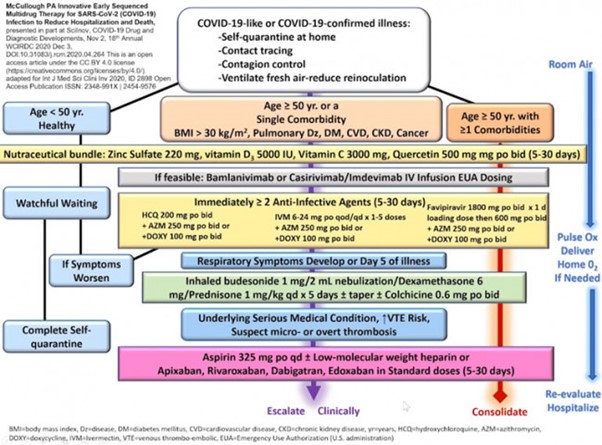
We synthesized this [treatment for Covid 19] into this protocol which is very comprehensive, and many could condense this, but once someone contracts Covid 19, the patient quarantines at home, we do contact tracing, the patient ventilates the room, and gets fresh air. If the patient age is under 50, we use just nutraceuticals: zinc sulfate (220 milligrams contains 50 milligrams of zinc) vitamin D3 5,000 units, vitamin C 3,000 milligrams, quercetin 500 milligrams twice a day. You could add lysine or n-acetylcysteine. Medical personnel maintain “watchful waiting,” maintain complete quarantine. Once recovered, the patient goes back to work, with no additional testing. Nothing else is needed.
If symptoms worsen, then we move into the treatment protocol. The treatment protocol for patients over 50 and persons with medical problems—that’s when the risk of hospitalization or death emerges, it’s more than one percent—we use antibodies, if we can get an antibody infusion. In the United States, they’re free. We just call the hospital and have the patients go in, then we can use our two anti-infectives, hydroxychloroquine or ivermectin, or favipiravir outside the United States, plus azithromycin. We use inhaled budesonide throughout treatment now. If respiratory symptoms are there on day five, we give oral steroids. We use colchicine throughout, and then we use aspirin throughout, and then we can add the anticoagulants. So the physician can use this to integrate a program. It does not mean giving every drug for all patients, but we combine them.
We use home oxygen concentrators. I’ve treated people in their 90s at home, and they’ve gotten sick, but they have not been hospitalized. I’ve treated multiple families, people with oxygen saturations into the 70s, without them being hospitalized. It can be done at home because once the patient goes into the hospital in the United States, they get worse care. We can actually do much better in treating patients at home using these drugs. So fortunately, in the United States we can do this now…
In 849 PCR-positive high-risk patients we demonstrated about an 85% reduction in hospitalization and death, and the combinations are all a little bit different over time, but the point is to use the drugs in combination. There are no randomized trials that use four to six drugs in combination versus matching placebos, and there are no randomized trials planned, so this idea that we’re going to wait for randomized trials is not supportable because we don’t have the randomized trials that are even planned. This is the best we can do. If we add in the data from Dr. Raoult, Dr. Milan and Dr. Zelenko, we have a very strong body of evidence to show that we can use drugs in combination—very strong…
Problems with the Regulation and Surveillance of Vaccination Programs
The vaccine programs [in the United States] do not have critical event committees, data safety monitoring reports, or ethics committees. The programs are not safe. They’re not safe like a clinical trial because they don’t have the safety mechanisms, and this paper basically says if the vaccine programs cannot get safety mechanisms in place, they should shut down. The concern that we have is the mechanism of action of messenger RNA or adenoviral DNA is not safe. It causes uncontrolled production of the spike protein in cells and tissues. It causes endothelial damage. It causes the spike protein to get into the circulation and the body fluids. It is contaminating the donated blood supply. There are no genotoxicity studies, no teratogenicity studies [effects on the fetus]. There’s a very concerning biodistribution study from Pfizer showing it goes to the ovaries. There is a concerning fertility study of the Moderna vaccine showing reduced fertility. There’s no external event committee, no data safety monitor board or human ethics committee, and no restriction of properly excluded drugs. Pregnant women and women of childbearing potential, and covid survivors previously immune were not in the clinical trials. Under no circumstances should they be vaccinated. There has been no effort to restrict vaccination according to risk for Covid 19 hospitalization and death. This means people under age 50 have a minimal risk of hospitalization and death, so they should not be receiving the vaccine. There’s no attempt to present or mitigate risks to the public. We’ve been on TV now demanding that our authorities present the safety data because Americans are getting propaganda. They’re not getting fair information on safety.
We had an emerging safety signal in the United States on January 22nd, 2021 when we had vaccinated 27.1 million people. We had 182 vaccine deaths after Covid vaccines. From all the vaccines combined per year in the United States, there are about 158 deaths. That’s from 500 million shots and 72 different vaccines, and they’re not related in time to the injection. So we knew at 182 deaths by January 22nd that we had a mortality problem with the Covid 19 vaccines. You can see the big spike in death due to the vaccines, and it happened with the Covid 19 vaccines. This is an undeniable mortality signal. Undeniable.
Now as of June 11th, we have nearly 6,000 deaths. We have a concordant number of hospitalizations and clinic visits, and this far exceeds normal. We have a total of 358,000 safety reports. We normally get 16,000 safety reports a year, so it’s undeniable that we’ve got a major problem. When we look at the timing when these events occur, we know that 44% of the deaths occur within 48 hours of the vaccine, so the vaccine is playing a role in these deaths almost certainly. They appear to be acute allergic events in the two days afterward—what’s called reactogenic deaths, with fever and chills. The spike protein is damaging the organs, causing death after about two weeks from thrombocytopenic purpura, or cavernous venous thrombosis, and myocarditis. This has now been well described. All of these are adding to the terrible deaths that we’re seeing with Covid 19. So as we sit here today in the United States, there’s more vaccine injury and death than hospitalization and death due to the respiratory infection. The vaccine is causing more damage than the original problem.
Dr. Tess Lowry, who’s at the evidence-based consulting group in the UK and was a principal advisor to the World Health Organization, has stated that the vaccines are not safe for human use and she’s advised the British government to stop vaccination. Stop vaccination. Not safe. Take them off the market. Take them away from the public.
A New Safer Vaccine
Now the good news is it looks like a safer vaccine is coming. The Novavax vaccine looks quite good. This is just an antigen. It’s just the spike protein antigen. It is not a genetic vaccine. It does not create uncontrolled production of spike protein. It’s a limited amount of spike protein. They’re going to go with 5 micrograms. The safety profile shows almost no severe or life-threatening safety events, only mild or moderate events. The efficacy looks just as good as Pfizer and Moderna. Some countries still need to vaccinate older people. In the United States, 77 percent of people over age 65 are vaccinated. We have 45 percent of Americans vaccinated. That’s good enough, but some countries still need to vaccinate the older people, and we think Novavax would play a big role.
Conclusion
So to finish and conclude, the Covid 19 pandemic is a global disaster. Its pathophysiology is complex. It’s not amenable to a single drug. We need to use drugs in combination. Despite contagion control efforts, there are two bad outcomes: hospitalization and death. The pre-hospital phase is the time for therapeutic opportunity. Hospitalization in late treatment is an inadequate safety net, with unacceptably high mortality. In the United States, the current mortality rate for a hospitalized patient who needs the ICU (Intensive Care Unit) is 38 percent. It’s too high. Early ambulatory therapy with a sequenced multi-drug regimen is supported by available sources of evidence and has a positive benefit-to-risk profile. We just need to look for signals of benefit and acceptable safety. We’ve shown we can reduce hospitalization and death. We can more safely buy time until we can get to a safe vaccine. The Covid 19 genetic vaccines’ unfavorable safety profile cannot be generally supported in clinical practice at this time.
TRANSCRIPT (TRANSLATION / PARAPHRASE)
I can say that half of the cases of the Indian variant [delta variant] that we have identified are found in people who are vaccinated, so this variant’s potential is not negligible.
I continue to think that for those who are at high risk of severe infection or death, those over age 65, or those who are younger but vulnerable, for health care workers exposed to the virus, it is reasonable for them to be vaccinated, even if it only decreases the risk by 50-60%, a figure which has been demonstrated recently in Israel. It’s better than nothing, but we have to get away from this idea that the vaccine is going to resolve everything and the pandemic will be over. We have to use every tool at our disposal—early detection, early treatment, early surveillance, taking blood oxygen readings—things we do with other infectious diseases. We have to get back to doing medical care.
These vaccines [for SARS-Cov-2] are not like the vaccines for measles or smallpox, two diseases which we were able to eradicate. These vaccines for SARS-Cov-2 don’t provide immunity like the vaccines against those very stable viruses. I thought from the beginning that in France we should handle the coronavirus the way we handle annual influenza. We should have used inactivated viruses for the vaccines to which we could add adjuvants to increase their effectiveness. Then we could update them as new variants became apparent. We could do an annual vaccination, concentrating on those who are most vulnerable. We have to get back to this sensible approach.
The AstraZeneca vaccine is not recommended for women younger than fifty because there have been rates of thrombosis and death that are superior to that of the disease itself. Not only are women younger than fifty not fully protected from the disease by this vaccine, but the disease will not kill them, unless they have comorbidities.

Dear Dennis
Hello from the UK. Thank you for your post. However, I would point out that in fact none of the vaccines work to the benefit of physical health, and none of them ever have. I used to think otherwise until I carefully researched last year at 60 years of age.
We know that adverse effects happen with all vaccine some worse than others. The only question remains as to whether stimulating the immune system to elicit a response is of any benefit. Anti-bodies will be produced, but that is what a good immune system should do. These anti-bodies do not last that long.
The truth is we need to maintain a good immune system via, among other things, good levels of vitamins and minerals, key to which are vitamins D and C. These help our bodies deal with the toxicosis of our bodies which is what occurs when we have the ‘flu or Covid 19 as it is currently known.
I have written extensively regarding Covid 19 on my website and you may be interested to see my further reasoning in the following link.
Kind regards
Baldmichael Theresoluteprotector’sson
LikeLiked by 1 person
Hey! I could have sworn I’ve been to this blog before but after checking through some of the post I realized it’s new to me. Anyways, I’m definitely happy I found it and I’ll be book-marking and checking back often!
LikeLike