Medical Service Quality, Efficiency and Cost Control Effectiveness of Upgraded Case Payment in Rural China: A Retrospective Study


Abstract
:1. Introduction
2. Methods
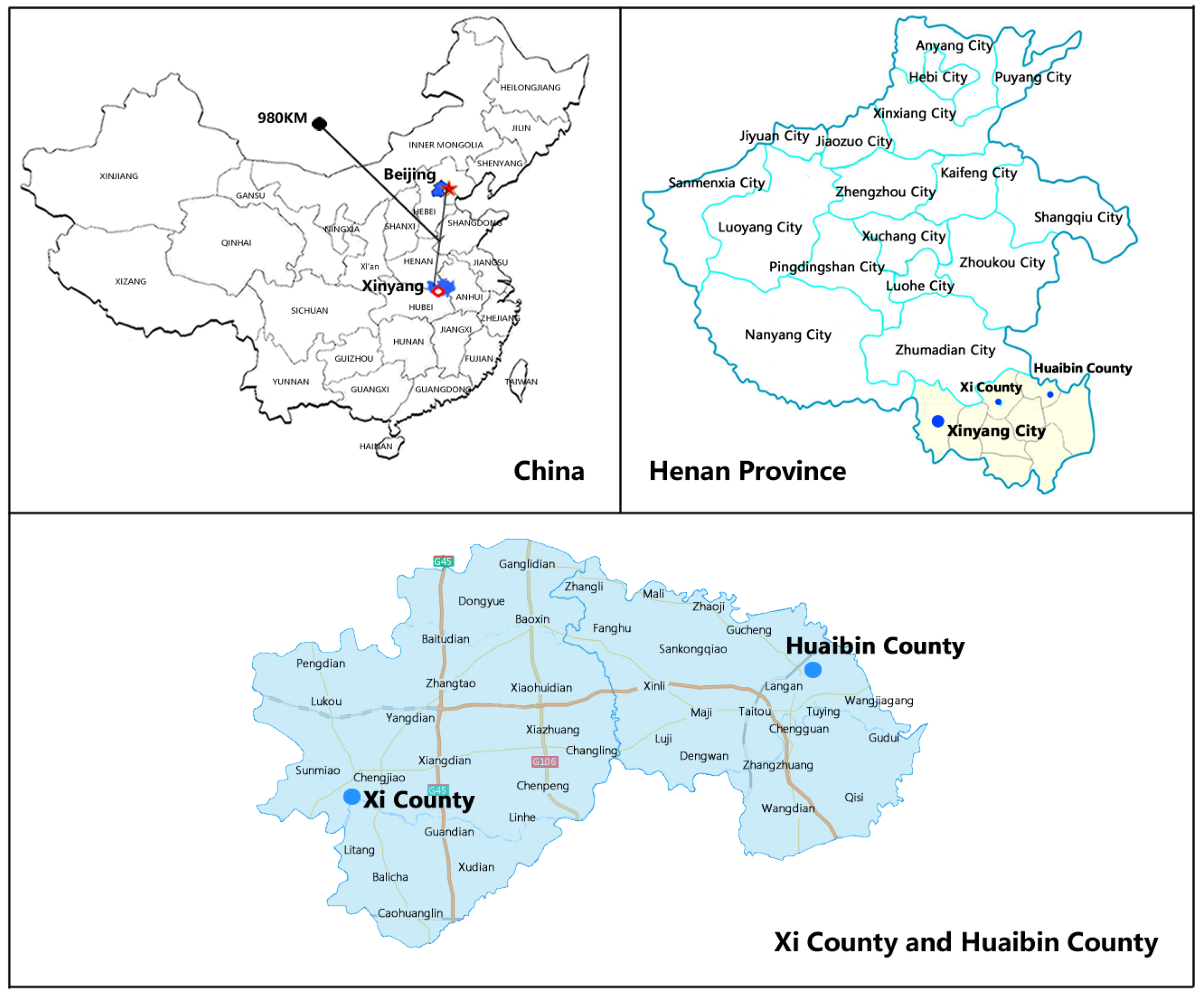
2.1. Study Setting and Intervention Assignment
2.2. Study Design and Variables
2.3. Statistical Analyses
2.4. Ethics Statement
3. Results
3.1. Study Sample Characteristics
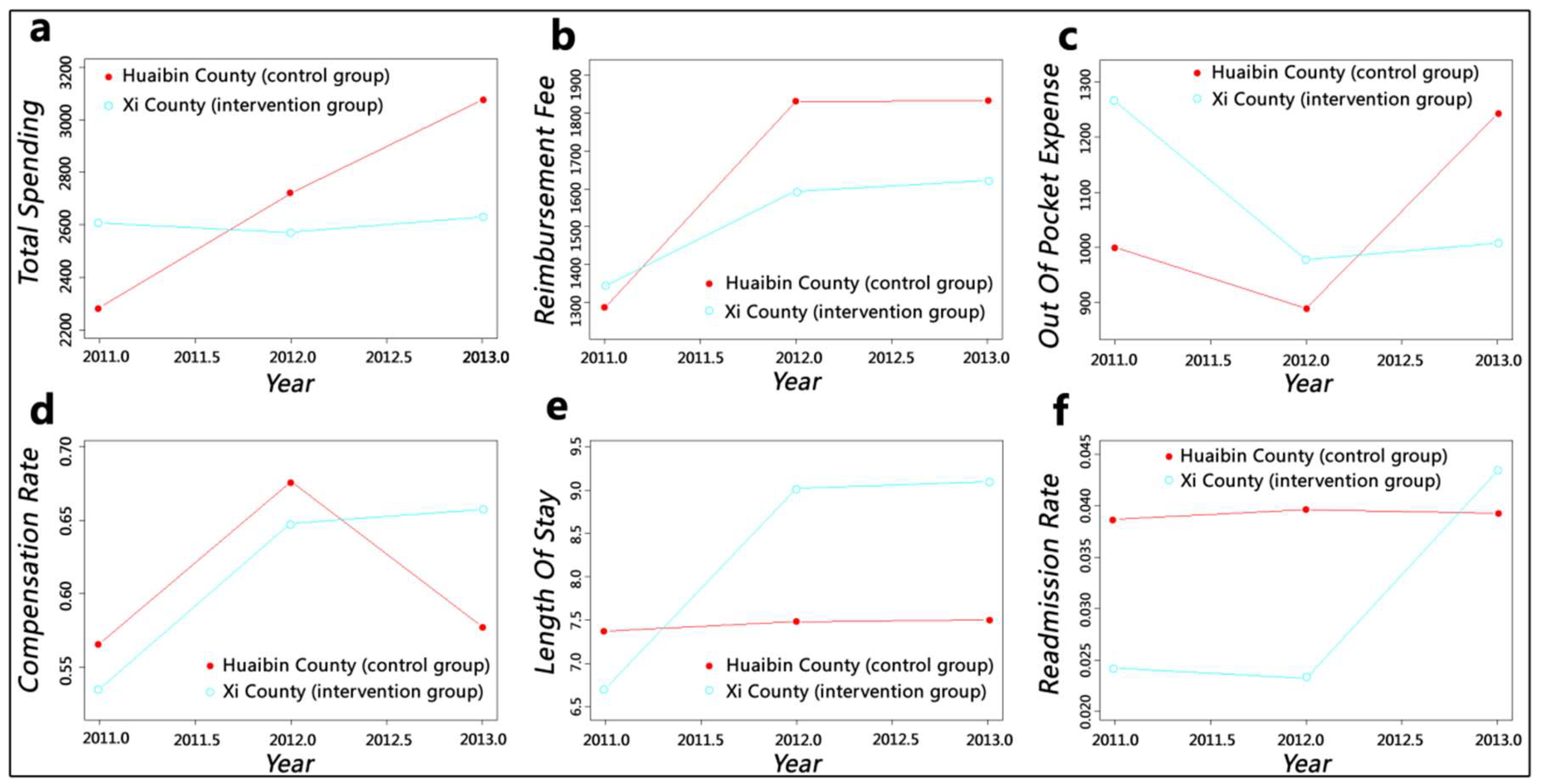
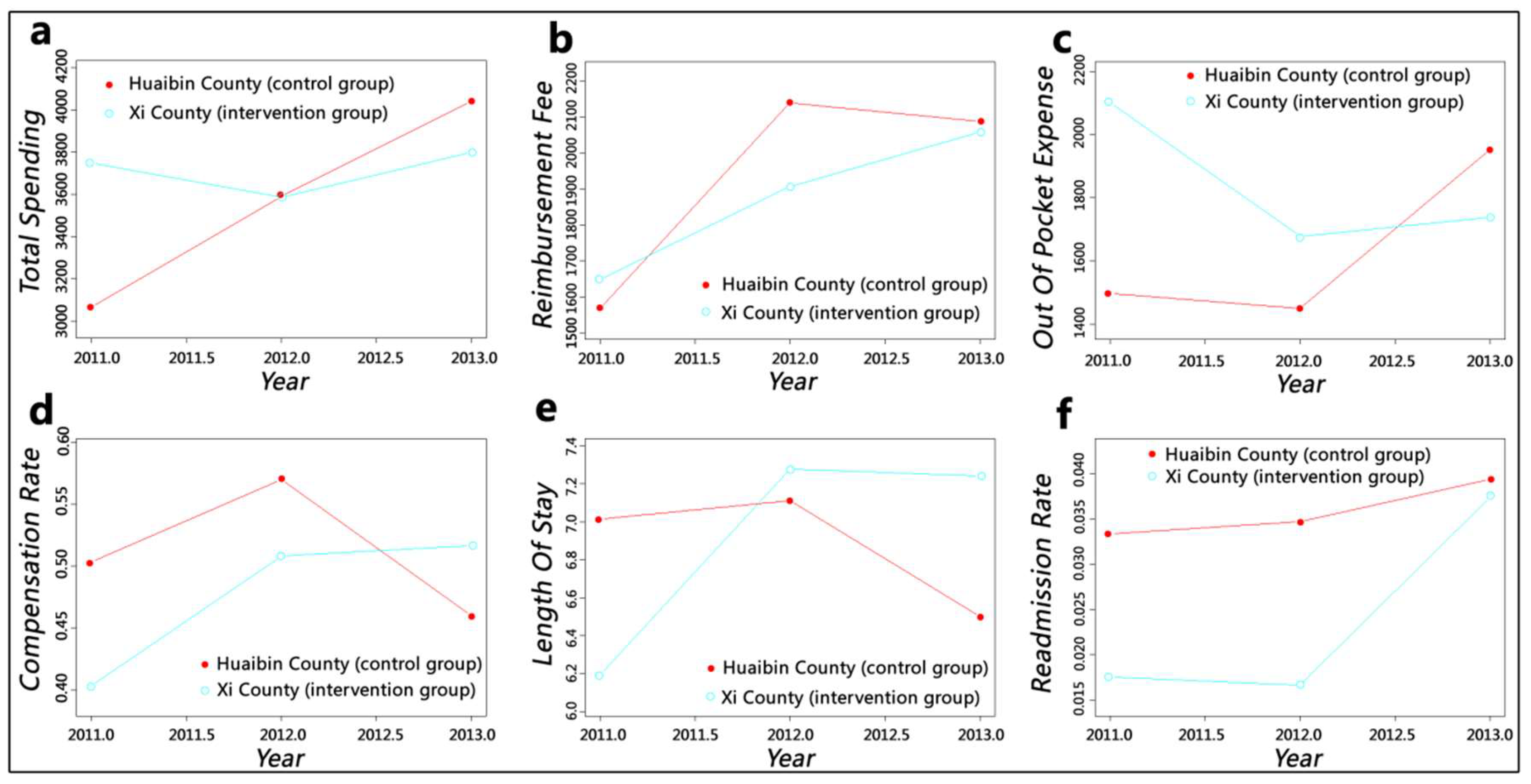
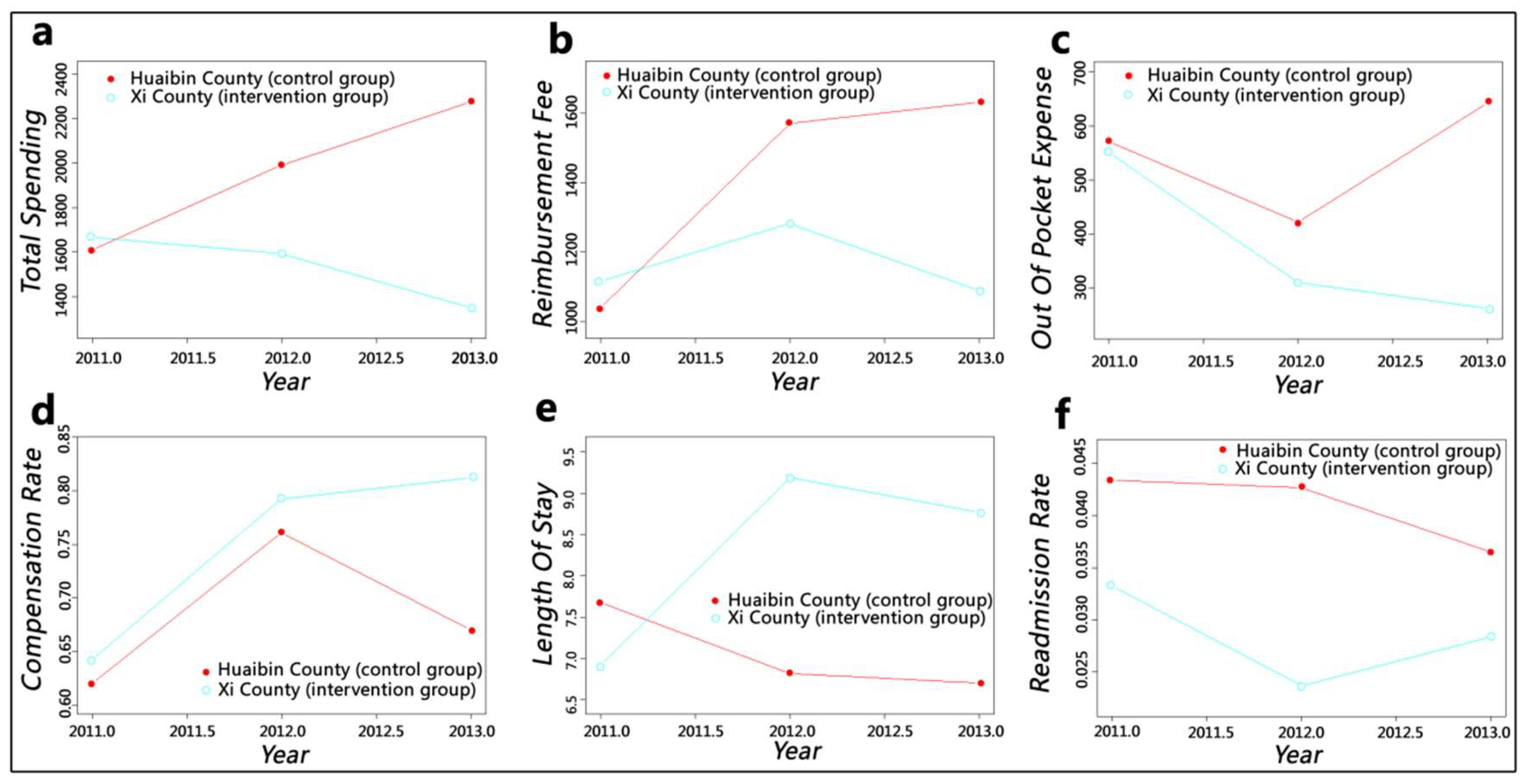
3.2. Policy Effects Shown by Observing Smooth Curve Trend
3.3. Policy Effects Observed from Difference-In-Differences Approach (DID) Model Outcomes
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Keehan, S.P.; Cuckler, G.A.; Sisko, A.M.; Madison, A.J.; Smith, S.D.; Stone, D.A.; Poisal, J.A.; Wolfe, C.J.; Lizonitz, J.M. National health expenditure projections, 2014–24: Spending growth faster than recent trends. Health Aff. 2015, 34, 1407–1417. [Google Scholar] [CrossRef] [PubMed]
- OECD. Health at a Glance 2017: OECD Indicators. 2017. Available online: http://dx.doi.org/10.1787/health_glance-2017-en (accessed on 10 November 2017).
- National Health and Family Planning Commission of the People’s Republic of China. China Health Statistical Yearbook 2017. Available online: http://www.yearbookchina.com/navibooklist-n2017120225-1.html (accessed on 1 September 2017). (In Chinese)
- Eggleston, K. Kan Bing Nan, Kan Bing Gui: Challenges for China’s Healthcare System Thirty Years into Reform; Walter, H. Shorenstein Asia-Pacific Research Center: Stanford, CA, USA, 2010. [Google Scholar]
- Zhao, C.R.; Wang, C.; Shen, C.W.; Wang, Q. Diagnosis-related group (DRG)-based case-mix funding system, a promising alternative for fee for service payment in China. Biosci. Trends 2018, 12, 109–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busse, R.; Schreyögg, J.; Smith, P.C. Hospital case payment systems in Europe. Health Care Manag. Sci. 2006, 9, 211–213. [Google Scholar] [CrossRef] [PubMed]
- Hwang, C.J.; See, L.C.; Chuang, Y.C. Case Payment and the Adoption of New Technology: An Empirical Study of Cataract Surgery in Taiwan. Chang Gung Med. J. 2004, 27, 327–336. [Google Scholar] [PubMed]
- Salkever, D.S.; Steinwachs, D.M.; Rupp, A. Hospital cost and efficiency under per service and per case payment in Maryland: A tale of the carrot and the stick. Inquiry 1986, 23, 56–66. [Google Scholar] [PubMed]
- Cheng, Y.L.; Chen, Y.C. Application Research of the Clinical Pathway in Single Disease Payment. Med. Soc. 2012, 25, 50–52. (In Chinese) [Google Scholar]
- Tan, Y.Q.; Xiang, L.; Xiong, J.Y.; Chen, Y.; Yao, L. A study on the limiting expenses payment of a single disease in Qianjiang district Chongqing city. Chin. J. Health Policy 2009, 2, 14–17. (In Chinese) [Google Scholar]
- Lang, H.C.; Chi, C.; Liu, C.M. Impact of the case payment reimbursement method on the utilization and costs of laparoscopic cholecystectomy. Health Policy 2004, 67, 195–206. [Google Scholar] [CrossRef]
- Quinn, K. After the revolution: DRGs at age 30. Ann. Intern. Med. 2014, 160, 426–429. [Google Scholar] [CrossRef]
- Reid, B.; Palmer, G.; Aisbett, C. The performance of Australian DRGs. Aust. Health Rev. 2000, 23, 20–31. [Google Scholar] [CrossRef] [Green Version]
- Okamura, S.; Kobayashi, R.; Sakamaki, T. Case-mix payment in Japanese medical care. Health Policy 2005, 74, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Xu, X.H.; Liu, G.M.; Xiang, G.P. Brief introduction of medical insurance system in China. Asia Pac. J. Oncol. Nurs. 2016, 3, 51. [Google Scholar] [CrossRef] [PubMed]
- He, R.B.; Miao, Y.D.; Ye, T.; Zhang, Y.; Tang, W.X.; Zhang, L. The effects of global budget on cost control and readmission in rural China: A difference-in-difference analysis. J. Med. Econ. 2017, 20, 903–910. [Google Scholar] [CrossRef] [PubMed]
- National Health Commission of the People’s Republic of China. Circular on the Pilot Work of Case Based Payment. 2004. Available online: http://www.moh.gov.cn/mohghcws/s3582/200804/16422.shtml (accessed on 17 August 2004). (In Chinese)
- National Development and Reform Commission. Circular on the Promoting the Case Based Payment. 2017. Available online: http://www.ndrc.gov.cn/zcfb/zcfbtz/201701/t20170116_835180.html (accessed on 10 January 2017). (In Chinese)
- General Office of the State Council. Guidance on Further Deepening the Reform of Basic Medical Insurance Payment. 2017. Available online: http://www.gov.cn/zhengce/content/2017-06/28/content_5206315.htm (accessed on 28 June 2017). (In Chinese)
- Jin, P.Y.; Biller-Andorno, N.; Wild, V. Ethical Implications of Case-Based Payment in China: A Systematic Analysis. Dev. World Bioeth. 2015, 15, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Wang, J.; Zhang, L.; Zhang, X. Caesarean section rate and cost control effectiveness of case payment reform in the new cooperative medical scheme for delivery: Evidence from Xi County, China. BMC Pregnancy Childbirth 2018, 18, 66. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.Z.; Liu, G.X.; Gao, X.; Lv, L.L. Research on the Implementation of Single-DRGs Reform under Chinese New Rural Cooperative Medical System. Chin. Health Econ. 2013, 32, 47–49. (In Chinese) [Google Scholar]
- Xie, L.; Wang, H.P.; Zhou, L.L.; Zhong, X.X.; Ding, H. Analysis on the composition and influencing factors of coronary heart disease patients’ hospitalization expenses under DRGs in Anhui Province. Chin. J. Health Policy 2018, 11, 70–73. (In Chinese) [Google Scholar]
- Jin, P.Y.; Biller-Andorno, N.; Wild, V. Case-Based Payment System in the Chinese Healthcare Sector and Its Ethical Tensions. Asian Bioeth. Rev. 2013, 5, 131–146. [Google Scholar]
- Cheng, N.; Wang, Z.L.; Fu, X.G.; Song, D.P.; Ren, J.; Zhao, D.H. Analysis on the Results of Medical Expense Control and Influencing Factors in Typical Regions of Payment Reforms under New Rural Cooperative Medical System. Chin. Health Econ. 2017, 36, 32–35. (In Chinese) [Google Scholar]
- Li, Y.; Yang, W.; He, R.B.; Zhang, L. Thoughts and Practice of DRGs-Based Multi-Faceted Payment Reform in Xixian, Henan Province. Chin. Health Econ. 2017, 36, 36–38. (In Chinese) [Google Scholar]
- Shi, L.Y.; Makinen, M.; Lee, D.C.; Kidane, R.; Blanchet, N.; Liang, H.; Li, J.; Lindelow, M.; Wang, H.; Xie, S.; et al. Integrated care delivery and health care seeking by chronically-ill patients—A case-control study of rural Henan province, China. Int. J. Equity Health 2015, 14, 98. [Google Scholar] [CrossRef] [PubMed]
- Shi, M.; Wang, J.; Zhang, L.; Yan, Y.; Miao, Y.D.; Zhang, X. Effects of Integrated Case Payment on Medical Expenditure and Readmission of Inpatients with Chronic Obstructive Pulmonary Disease: A Nonrandomized, Comparative Study in Xi County, China. Curr. Med. Sci. 2018, 38, 558–566. [Google Scholar] [CrossRef] [PubMed]
- The World Bank. China-Rural Health Project. 2008. Available online: http://projects.worldbank.org/P084437/rural-health-project?lang=en (accessed on 24 December 2014).
- Sheynin, O.B. Studies in the history of probability and statistics. XXI. On the early history of the law of large numbers. Biometrika 1968, 5, 59–67. [Google Scholar] [CrossRef]
- Yip, W.C.; Wang, H.; Liu, Y. Determinants of patient choice of medical provider: A case study in rural China. Health Policy Plan. 1998, 13, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.T.; Wu, Q.H.; Li, Y.; Hao, Y.H.; Huang, Z.Q.; Jiao, M.L.; Liang, L.B.; Kang, Z. Analysis of the Change Tendency of Inpatient Flow and Hospital Cost Burden Among Rural Residents Under New Rural Cooperative Medical Scheme. Chin. Hosp. Manag. 2015, 35, 72–74. (In Chinese) [Google Scholar]
- Yang, Y.; Ning, J.G.; Zhao, J.; Xiong, L.P. Analyzing the status of hospitalization of insured in the New Rural Cooperative Medical System in different medical institutions. Chin. Health Serv. Manag. 2015, 32, 135–137. (In Chinese) [Google Scholar]
- Jin, T.J.; Chen, Y.C.; Wu, N.N.; Zhang, L.J.; Li, H.M.; Shi, L.Q.; Zhang, Y. Analysis on the Effects of the Adjusting the Hospitalized Distribution of Patients outside the County on the New Rural Cooperative Medical System Fund and the Resident Compensation Beneficiary: Taking a County of Hubei as Case Study. Chin. Health Econ. 2015, 34, 36–39. (In Chinese) [Google Scholar]
- DiMatteo, M.R.; Sherbourne, C.D.; Hays, R.D.; Ordway, L.; Kravitz, R.L.; McGlynn, E.A.; Kaplan, S.; Rogers, W.H. Physicians’ characteristics influence patients’ adherence to medical treatment: Results from the Medical Outcomes Study. Health Psychol. 1993, 12, 93. [Google Scholar] [CrossRef]
- Zhang, Y.T.; Ma, Q.H.; Chen, Y.C.; Gao, H.X. Effects of public hospital reform on inpatient expenditures in rural China. Health Econ. 2017, 26, 421–430. [Google Scholar] [CrossRef]
- Abadie, A. Semiparametric difference-in-differences estimators. Rev. Econ. Stud. 2005, 72, 1–19. [Google Scholar] [CrossRef]
- Hastie, T.; Tibshirani, R. Generalized Additive Models. Stat. Sci. 1986, 1, 297–310. [Google Scholar] [CrossRef] [Green Version]
- Guisan, A.; Edwards, T.C., Jr.; Hastie, T. Generalized linear and generalized additive models in studies of species distributions: Setting the scene. Ecol. Model. 2002, 157, 89–100. [Google Scholar] [CrossRef]
- Li, H.M.; Chen, Y.C.; Gao, H.X.; Zhang, Y.; Chen, L.; Chang, J.J.; Su, D.; Lei, S.H.; Jiang, D.; Hu, X.M. Effectiveness evaluation of quota payment for specific diseases under global budget: A typical provider payment system reform in rural China. BMC Health Serv. Res. 2018, 18, 635. [Google Scholar] [CrossRef] [PubMed]
- Ke, H.; Ma, J.; Zhang, F. The Application of Generalize Additive Models in Medical Cost Control. Chin. J. Health Stat. 2012, 29, 833–836. (In Chinese) [Google Scholar]
- National Bureau of Statistics of the People’s Republic of China. China Statistical Yearbook. 2014. Available online: http://data.stats.gov.cn/easyquery.htm?cn=C01&zb=A090305&sj=2017 (accessed on 1 September 2014).
- Ding, R.; Ji, J.P.; Gao, G.Y.; Zhang, Y.; Liu, S.P. Reflecting on the Factors Contributing to the Fund Overspending of the Cooperative Medical Scheme in Beijing and the Solutions to the Problem. Chin. Health Econ. 2012, 31, 38–40. (In Chinese) [Google Scholar]
- Ren, G.; Wang, Z.L. Empirical Analysis of the Reasons for Fund Cost Overruns of the New Rural Cooperative Medical Scheme. Chin. Health Econ. 2012, 31, 43–45. (In Chinese) [Google Scholar]
- Li, Z.; Yang, J.; Wu, Y.; Pan, Z.J.; He, X.Q.; Zhang, L. Challenges for the surgical capacity building of township hospitals among the Central China: A retrospective study. Int. J. Equity Health 2018, 17, 55. [Google Scholar] [CrossRef]
- Ji, X.R.; Wang, L.S. Analysis on Bed Utilizition Rate of County Level Hospitals in Central and Western Region. Chin. Health Econ. 2010, 29, 21–24. (In Chinese) [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indicators | Xi County | Huaibin County |
|---|---|---|
| Location | Contiguous to Huaibin | Contiguous to Xi |
| Administrative districts | 21 | 19 |
| Urbanization rate (%) | 35.7 | 36.2 |
| Permanent resident population (thousand) | 833.5 | 565.7 |
| Per capita annual income (yuan) | 13,235 | 12,946 |
| Number of county-level hospitals | 3 | 3 |
| Number of township hospitals | 20 | 19 |
| Number of hospital beds (per thousand population) | 2.05 | 2.38 |
| Number of practitioners (per thousand population) | 1.36 | 1.48 |
| Number of nurses (per thousand population) | 1.07 | 1.11 |
| Baseline (2011) | Follow-Up (2013) | |||||
|---|---|---|---|---|---|---|
| Xi (Intervention) | Huaibin (Control) | p | Xi (Intervention) | Huaibin (Control) | p | |
| N | 36,104 | 33,073 | 59,087 | 51,325 | ||
| Gender | <0.001 | <0.001 | ||||
| Male | 15,173 (42.03%) | 14,270 (43.15%) | 25,816 (43.69%) | 21,577 (42.04%) | ||
| Female | 20,931 (57.97%) | 18,803 (56.85%) | 33,271 (56.31%) | 29,748 (57.96%) | ||
| Age group | <0.001 | <0.001 | ||||
| 0–17 | 4897 (13.56%) | 2944 (8.90%) | 6630 (11.22%) | 3887 (7.57%) | ||
| 18–34 | 9973 (27.62%) | 6605 (19.97%) | 12,711 (21.51%) | 11,388 (22.19%) | ||
| 35–64 | 13,477 (37.33%) | 15,554 (47.03%) | 23,820 (40.31%) | 23,078 (44.96%) | ||
| ≥65 | 7757 (21.49%) | 7970 (24.09%) | 15,926 (26.95%) | 12,972 (25.27%) | ||
| Institution level | <0.001 | <0.001 | ||||
| Township level | 17,921 (49.64%) | 19,179 (57.99%) | 24,788 (41.95%) | 25,212 (49.12%) | ||
| County level | 18,183 (50.36%) | 13,894 (42.01%) | 34,299 (58.05%) | 26,113 (50.88%) | ||
| Total spending (¥) | 2451.26 | 2103.90 | <0.001 | 2690.09 | 3066.93 | <0.001 |
| Reimbursement fee (¥) | 1302.53 | 1264.99 | <0.001 | 1841.45 | 1898.87 | <0.001 |
| Out-of-pocket expense (¥) | 1148.73 | 838.91 | <0.001 | 848.65 | 1168.06 | <0.001 |
| Compensation ratio (%) | 54.27 | 59.17 | <0.001 | 69.46 | 59.18 | <0.001 |
| Length of stay (days) | 7.05 | 7.71 | 0.558 | 9.43 | 7.85 | <0.001 |
| Readmission | <0.001 | <0.001 | ||||
| No | 35,006 (96.96%) | 31,492 (95.22%) | 55,853 (94.53%) | 48,804 (95.09%) | ||
| Yes | 1098 (3.04%) | 1581 (4.78%) | 3234 (5.47%) | 2521 (4.91%) | ||
| Outcome Variable | 2011 (Baseline) | 2013 (Follow-up) | Difference-in-Differences | ||||
|---|---|---|---|---|---|---|---|
| Intervention | Control | Difference | Intervention | Control | Difference | ||
| Whole county | |||||||
| Total spending | 1602.12 | 1180.07 | 422.04 *** | 2212.46 | 2137.01 | 75.45 *** | −346.59 *** |
| Reimbursement fee | 615.03 | 513.20 | 101.83 *** | 1137.61 | 1141.17 | −3.56 | −105.39 *** |
| Out of pocket expense | 987.09 | 666.87 | 320.21 *** | 1074.85 | 995.84 | 79.01 *** | −241.20 *** |
| Compensation rate | 0.448 | 0.487 | −0.039 *** | 0.517 | 0.486 | 0.031 *** | 0.070 *** |
| Length of stay | 3.41 | 4.08 | −0.67 *** | 4.89 | 3.38 | 1.51 *** | 2.18 *** |
| Readmission rate | 0.013 | 0.028 | −0.016 *** | 0.029 | 0.030 | −0.001 | 0.015 *** |
| County hospital | |||||||
| Total spending | 1629.48 | 938.26 | 691.22 *** | 1666.02 | 1917.94 | −251.92 *** | −943.14 *** |
| Reimbursement fee | 440.97 | 361.51 | 79.46 *** | 815.77 | 886.47 | −70.70 *** | −150.16 *** |
| Out-of-pocket expense | 1188.51 | 576.75 | 611.75 *** | 850.25 | 1031.47 | −181.22 *** | −792.97 *** |
| Compensation rate | 0.397 | 0.497 | −0.100 *** | 0.498 | 0.454 | 0.044 *** | 0.144 *** |
| Length of stay | 1.52 | 2.30 | −0.78 *** | 2.30 | 1.84 | 0.46 *** | 1.24 *** |
| Readmission rate | 0.005 | 0.025 | −0.020 *** | 0.046 | 0.034 | 0.013 *** | 0.033 *** |
| Township health centre | |||||||
| Total spending | 1124.59 | 1073.83 | 50.76 *** | 566.08 | 1735.87 | −1169.79 *** | −1220.55 *** |
| Reimbursement fee | 605.99 | 534.28 | 71.71 *** | 379.19 | 1125.70 | −746.51 *** | −818.22 *** |
| Out-of-pocket expense | 518.60 | 539.54 | −20.94 *** | 186.89 | 610.17 | −423.28 *** | −402.34 *** |
| Compensation rate | 0.558 | 0.536 | 0.022 *** | 0.745 | 0.587 | 0.159 *** | 0.137 *** |
| Length of stay | 3.17 | 3.87 | −0.70 *** | 6.66 | 2.91 | 3.75 *** | 4.45 *** |
| Readmission rate | 0.019 | 0.030 | −0.011 *** | 0.008 | 0.027 | −0.016 *** | −0.005 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, R.; Ye, T.; Wang, J.; Zhang, Y.; Li, Z.; Niu, Y.; Zhang, L. Medical Service Quality, Efficiency and Cost Control Effectiveness of Upgraded Case Payment in Rural China: A Retrospective Study. Int. J. Environ. Res. Public Health 2018, 15, 2839. https://doi.org/10.3390/ijerph15122839
He R, Ye T, Wang J, Zhang Y, Li Z, Niu Y, Zhang L. Medical Service Quality, Efficiency and Cost Control Effectiveness of Upgraded Case Payment in Rural China: A Retrospective Study. International Journal of Environmental Research and Public Health. 2018; 15(12):2839. https://doi.org/10.3390/ijerph15122839
Chicago/Turabian StyleHe, Ruibo, Ting Ye, Jing Wang, Yan Zhang, Zhong Li, Yadong Niu, and Liang Zhang. 2018. "Medical Service Quality, Efficiency and Cost Control Effectiveness of Upgraded Case Payment in Rural China: A Retrospective Study" International Journal of Environmental Research and Public Health 15, no. 12: 2839. https://doi.org/10.3390/ijerph15122839