
Cell Phone Radiation Exposure Limits and Engineering Solutions
 , , , , , ,
, , , , , ,  and
and
Abstract
:
1. Introduction
2. Analysis
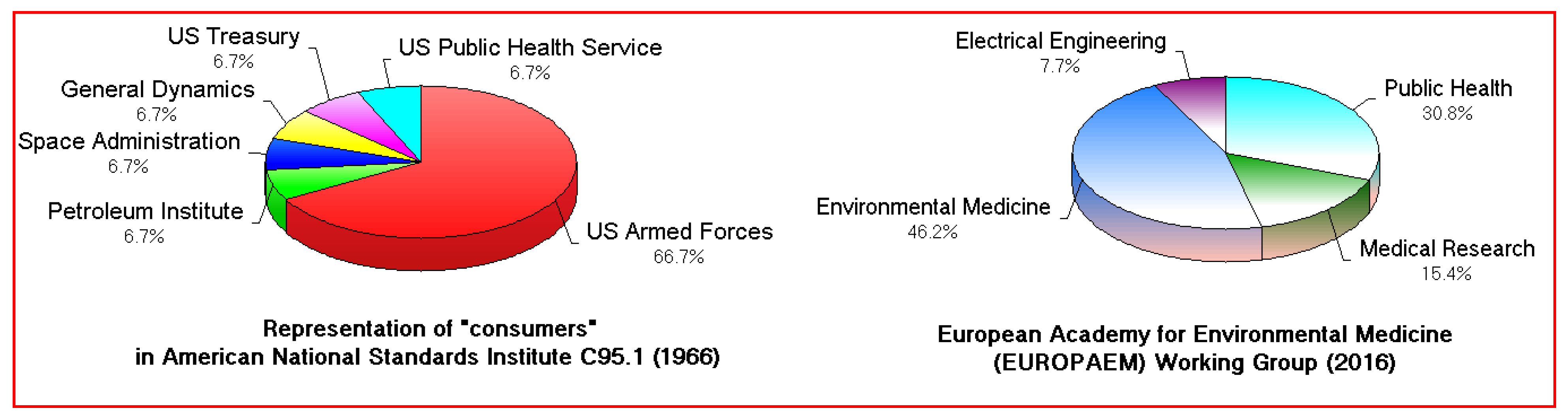
2.1. Blind Spot #1: RFR Toxicology and Risk Assessment
2.2. Blind Spot #2: 40–60 Min Is Not a Lifetime
2.3. Blind Spot #3: Averaging Human Exposures over 6 or 30 Min

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biological Events | Execution Time (s) |
|---|---|
| Individual charge transfer jumps | |
| Electron and Hole Transfer steps of photosynthesis in Photosystem II [47] | 3 × 10−12 2 × 10−10 0.1–2 × 10−7 10−4 0.1–2 × 10−3 10−2 |
| Electron and Proton translocations in oxidative phosphorylation Complex IV, cytochrome c oxidase [48] | 6 × 10−5 10−3 10−2 |
| Enzymatic reaction times from turnover numbers (substrate) [49] | |
| Carbonic Anhydrase (CO2) | 2.5 × 10−6 |
| Fumarase (Fumarate de- and hydration) | 1.25 × 10−3 |
| Ribonuclease (RNA degradation) | 1.26 × 10−3 |
| Tyrosyl-tRNA synthetase (Transfer RNA) | 0.13 |
| Pepsin (Protein degradation) | 2 |
| Chymotrypsin (Peptide bonds) | 7.14 |
| IEEE RFR integration time | 360 or 1800 (6 or 30 min) |
2.4. Blind Spot #4: RFR’s Human Costs
2.4.1. Cancer
2.4.2. Electromagnetic Hypersensitivity
2.5. Blind Spot #5: Specific Absorption Rates Determined at Unrealistic Distances
2.6. Blind Spot #6: Specific Absorption Rates Averaged over 1 or 10 g
2.7. Blind Spot #7: Enclosing the RFR Source
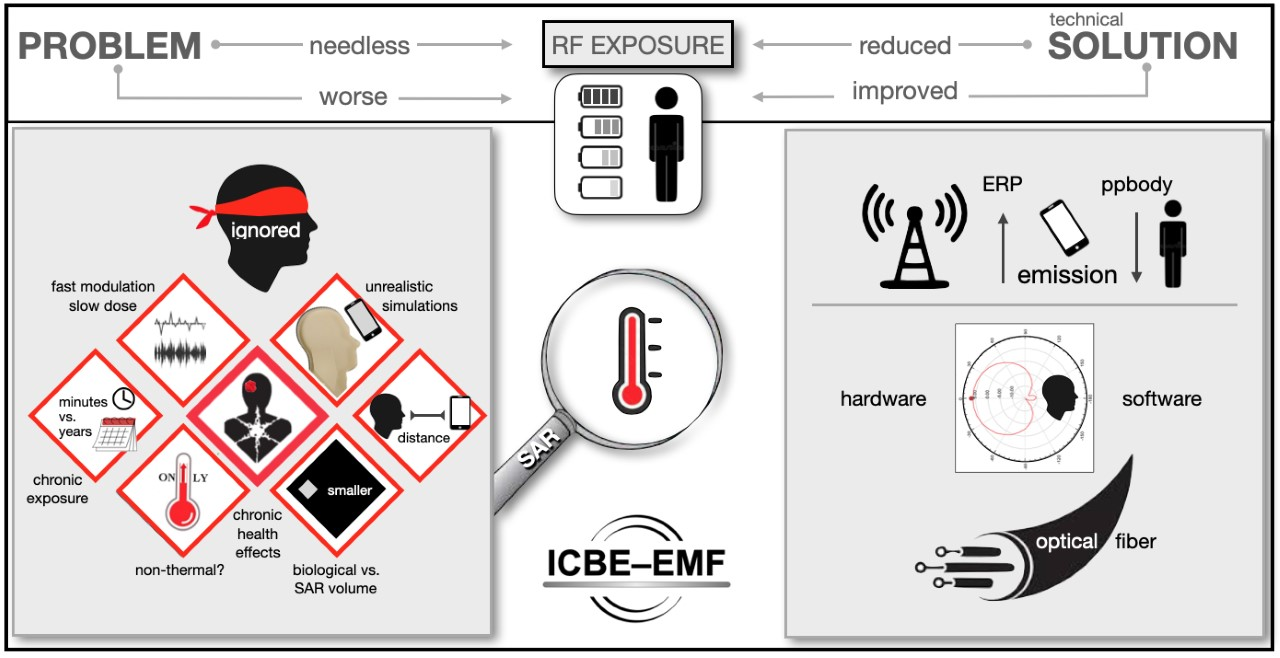
2.8. Blind Spots Summary
2.9. Engineering Solutions
- Blocking the phone’s RFR emissions, but not its reception, when it is positioned close to the head/body.
- Modifying the antenna emission pattern (to hemispherical) to radiate away from the head and the body.
- Limiting call durations according to an estimation of the effective radiated power emitted by the antenna over a specific period.
2.9.1. Cell Phone Emission Blocking
2.9.2. Improved Antennas
2.9.3. Improved Communication Procedures
2.9.4. Limiting Call Durations
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anghileri, L.J.; Robert, J. Hyperthermia in Cancer Treatment; CRC Press: Boca Raton, FL, USA, 1986; Volumes I–III. [Google Scholar]
- Laidler, K.J. The World of Physical Chemistry; Oxford University Press: Oxford, UK, 1993. [Google Scholar]
- Justesen, D.R. Toward a Prescriptive Grammar for the Radiobiology of Non-Ionising Radiations: Quantities, Definitions, and Units of Absorbed Electromagnetic Energy—An Essay. J. Microw. Power 1975, 10, 343–356. [Google Scholar] [CrossRef]
- Frey, A.H. On the Nature of Electromagnetic Field Interactions with Biological Systems; R. G. Landes Co.: Austin, TX, USA, 1994. [Google Scholar]
- Std C95.1-2005; IEEE Standard for Safety Levels with Respect to Human Exposure to Radio Frequency Electromagnetic Fields, 3 kHz to 300 GHz. IEEE: New York, NY, USA, 2006; p. 2.
- International Commission on Non-Ionizing Radiation Protection. Guidelines for limiting exposure to time-varying electric, magnetic, and electromagnetic fields (up to 300 GHz). Health Phys. 1998, 74, 494–522. [Google Scholar]
- International Commission on Non-Ionizing Radiation Protection. ICNIRP statement on the Guidelines for limiting exposure to time-varying electric, magnetic, and electromagnetic fields (up to 300 GHz). Health Phys. 2009, 97, 257–258. [Google Scholar] [CrossRef]
- International Commission on Non-Ionizing Radiation Protection. Guidelines for limiting exposure to electromagnetic fields (100 kHz to 300 GHz). Health Phys. 2020, 118, 483–524. [Google Scholar] [CrossRef] [PubMed]
- Wood, G. “The human body is already ionized”. Comment by Rep. Dr. Gary Woods, retired physicist and hand surgeon, speaker of the house appointee to the New Hampshire Commission to Study the Environmental and Health Effects of Evolving 5G Technology, during the New Hampshire 5G Commission Meeting of the 21st of November 2019.
- Mitchell, P. Chemiosmotic Coupling in Oxidative and Photosynthetic Phosphorylation. Biol. Rev. 1966, 41, 445–502. [Google Scholar] [CrossRef] [PubMed]
- Sanders, A.P.; Schaefer, D.J.; Joines, W.T. Microwave Effects on Energy Metabolism of Rat Brain. Bioelectromagnetics 1980, 1, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Sanders, A.P.; Joines, W.T.; Allis, J.W. Effects of Continuous-Wave, Pulsed, and Sinusoidal-Amplitude-Modulated Microwaves on Brain Energy Metabolism. Bioelectromagnetics 1985, 6, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Belyaev, I. Biophysical Mechanisms for Nonthermal Microwave Effects. In Electromagnetic Fields in Biology and Medicine; Markov, M., Ed.; CRC Press: Boca Raton, FL, USA; London, UK; New York, NY, USA, 2015. [Google Scholar]
- Belyaev, I. Main Regularities and Health Risks from Exposure to Non-Thermal Microwaves of Mobile Communication. In 2019 14th International Conference on Advanced Technologies, Systems and Services in Telecommunications (TELS IKS 2019), Proceedings of the 14th International Conference on Advanced Technologies, Systems and Services in Telecommunications (TELSIKS), Nis, Serbia, 23–25 October 2019; Milovanovic, B.D., Ed.; IEEE: New York, NY, USA, 2019; pp. 111–116. [Google Scholar]
- Jaffe, R.L. Degenerate Fermion Systems Lecture Notes 8.322 Quantum Theory II-2006; Massachusetts Institute of Technology: Cambridge, MA, USA, 2006; p. 113. [Google Scholar]
- Benabbas, A.; Salna, B.; Sage, J.T.; Champion, P.M. Deep proton tunneling in the electronically adiabatic and non-adiabatic limits: Comparison of the quantum and classical treatment of donor-acceptor motion in a protein environment. J. Chem. Phys. 2015, 142, 114101. [Google Scholar] [CrossRef]
- Slocombe, L.; Sacchi, M.; Al-Khalili, J. An open quantum systems approach to proton tunnelling in DNA. Commun. Phys. 2022, 5, 109. [Google Scholar] [CrossRef]
- ORSAA. Statement Regarding Harmful Biological Effects of Communication Radiofrequencies. 2021. Available online: https://www.orsaa.org/uploads/6/7/7/9/67791943/statemenbt_of_harm_march_2021-orsaa.pdf (accessed on 19 January 2023).
- BioInitiative Working Group. BioInitiative Report: A Rationale for Biologically-Based Public Exposure Standards for Electromagnetic Radiation; Sage, C., Carpenter, D.O., Eds.; BioInitiative: Gloucester, MA, USA, 2012; Available online: www.bioinitiative.org (accessed on 19 January 2023).
- Powell, R.M. Biological Effects from RF Radiation at Low-Intensity Exposure, Based on the BioInitiative 2012 Report, and the Implications for Smart Meters and Smart Appliances. 2013. Available online: https://www.emfanalysis.com/wp-content/uploads/2014/11/Powell-Bioinitiative-Report-Smart-Meters.pdf (accessed on 19 January 2023).
- Belyaev, I. Dependence of non-thermal biological effects of microwaves on physical and biological variables: Implications for reproducibility and safety standards. Eur. J. Oncol. Libr. 2010, 5, 187–218. [Google Scholar]
- Adey, W.R. Biological Effects of Electromagnetic Fields. J. Cell. Biochem. 1993, 51, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Georgiou, C.D. Oxidative Stress-Induced Biological Damage by Low-Level EMFs: Mechanism of Free Radical Pair Electron Spin-Polarization and Biochemical Amplification. In Non-Thermal Effects and Mechanisms of Interaction between Electromagnetic Fields and Living Matter; Giuliani, L., Soffritti, M., Eds.; Mattioli: Glasgow, UK, 2010; pp. 63–113. [Google Scholar]
- Yakymenko, I.; Sidorik, E.; Kyrylenko, S.; Chekhun, V. Long-term exposure to microwave radiation provokes cancer growth: Evidences from radars and mobile communication systems. Exp. Oncol. 2011, 33, 62–70. [Google Scholar]
- Yakymenko, I.; Tsybulin, O.; Sidorik, E.; Henshel, D.; Kyrylenko, O.; Kyrylenko, S. Oxidative mechanisms of biological activity of low-intensity radiofrequency radiation. Electromagn. Biol. Med. 2016, 35, 186–202. [Google Scholar] [CrossRef] [PubMed]
- Yakymenko, I.; Burlaka, A.; Tsybulin, O.; Brieieva, O.; Buchynska, L.; Tsehmistrenko, S.; Chekhun, V. Oxidative and mutagenic effects of low intensity GSM 1800 MHz microwave radiation. Exp. Oncol. 2018, 40, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.T.; Guyton, K.Z.; Gibbons, C.F.; Fritz, J.M.; Portier, C.J.; Rusyn, I.; De Marini, D.M.; Caldwell, J.C.; Kavlock, R.J.; Lambert, P.F.; et al. Key characteristics of carcinogens as a basis for organizing data on mechanisms of carcinogenesis. Environ. Health Perspect. 2016, 124, 713–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IARC. Non-Ionizing Radiation, Part 2: Radiofrequency Electromagnetic Fields. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans Volume 102. Available online: https://publications.iarc.fr/Book-And-Report-Series/Iarc-Monographs-On-The-Identification-Of-Carcinogenic-Hazards-To-Humans/Non-ionizing-Radiation-Part-2-Radiofrequency-Electromagnetic-Fields-2013 (accessed on 19 January 2023).
- IARC. Non-Ionizing Radiation, Part 1: Static and Extremely Low-frequency (ELF) Electric and Magnetic Fields. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans Volume 80. Available online: https://publications.iarc.fr/Book-And-Report-Series/Iarc-Monographs-On-The-Identification-Of-Carcinogenic-Hazards-To-Humans/Non-ionizing-Radiation-Part-1-Static-And-Extremely-Low-frequency-ELF-Electric-And-Magnetic-Fields-2002 (accessed on 19 January 2023).
- National Toxicology Program. Cell Phone Radio Frequency Radiation. 2019. Available online: https://ntp.niehs.nih.gov/whatwestudy/topics/cellphones/index.html (accessed on 19 January 2023).
- Falcioni, L.; Bua, L.; Tibaldi, E.; Lauriola, M.; De Angelis, L.; Gnudi, F.; Mandrioli, D.; Manservigi, M.; Manservisi, F.; Manzoli, I.; et al. Report of final results regarding brain and heart tumors in Sprague-Dawley rats exposed from prenatal life until natural death to mobile phone radiofrequency field representative of a 1.8 GHz GSM base station environmental emission. Environ. Res. 2018, 165, 496–503. [Google Scholar] [CrossRef]
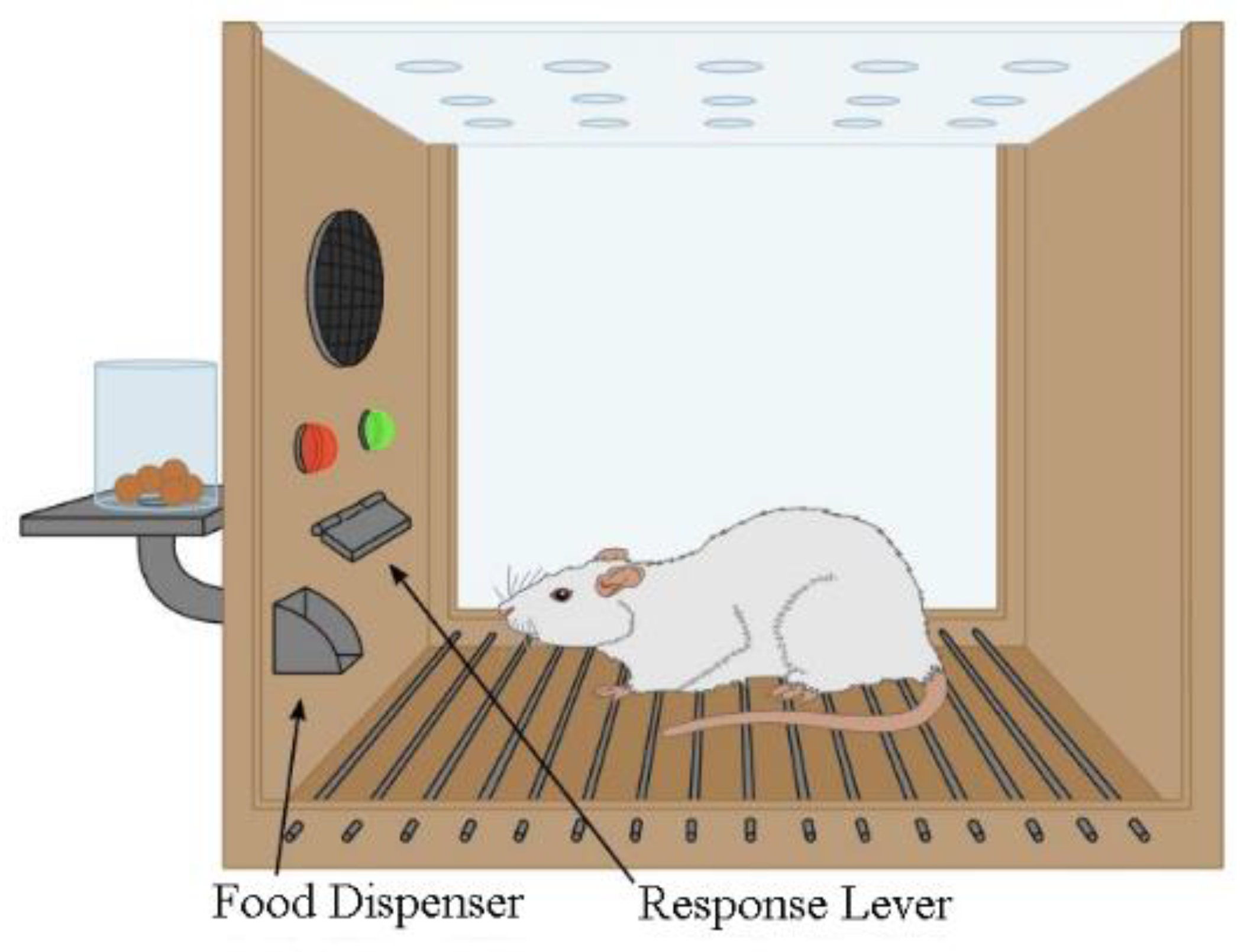
- de Lorge, J.O.; Ezell, C.S. Observing-responses of rats exposed to 1.28- and 5.62-GHz microwaves. Bioelectromagnetics 1980, 1, 183–198. [Google Scholar] [CrossRef]
- de Lorge, J.O. Operant behavior and colonic temperature of Macaca mulatta exposed to radio frequency fields at and above resonant frequencies. Bioelectromagnetics 1984, 5, 233–246. [Google Scholar] [CrossRef]
- Moser, V.C. Behavioral Screening for Toxicology. In Comprehensive Toxicology; Elsevier: Amsterdam, The Netherlands, 2010; pp. 337–350. [Google Scholar]
- U.S. Environmental Protection Agency. Toxic substances control act, test guidelines. Final Rule. 40 CFR, Part 798. Health effects testing guidelines. Subpart G-Neurotoxicity. Fed. Regist. 1985, 50, 39458–39470. [Google Scholar]
- Moser, V.C.; McCormick, J.P.; Creason, J.P.; MacPhail, R.C. Comparison of Chlordimeform and Carbaryl Using a Functional Observational Battery. Fundam. Appl. Toxicol. 1988, 11, 189–206. [Google Scholar] [CrossRef]
- Moser, V.C. Observational Batteries in Neurotoxicity Testing. Int. J. Toxicol. 2000, 19, 407–411. [Google Scholar] [CrossRef]
- Belyaev, I.; Dean, A.; Eger, H.; Hubmann, G.; Jandrisovits, R.; Kern, M.; Kundi, M.; Moshammer, H.; Lercher, P.; Müller, K.; et al. EUROPAEM EMF Guideline 2016 for the prevention, diagnosis and treatment of EMF-related health problems and illnesses. Rev. Environ. Health 2016, 31, 363–397. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Kim, Y.; Jeon, S.B.; Choi, H.D.; Lee, A.K.; Lee, H.J.; Pack, J.K.; Kim, N.; Ahn, Y.H. Effect of radiofrequency exposure on body temperature: Real-time monitoring in normal rats. J. Therm. Biol. 2022, 110, 103350. [Google Scholar] [CrossRef] [PubMed]
- Gad, S.C. Maximum Tolerated Dose. In Encyclopedia of Toxicology, 3rd ed.; Wexler, P., Ed.; Elsevier Reference Collection in Biomedical Sciences: Amsterdam, The Netherlands, 2014; p. 164. Available online: https://www.elsevier.com/books/encyclopedia-of-toxicology/wexler/978-0-12-386454-3 (accessed on 19 January 2023).
- Steneck, N.H. The Microwave Debate; MIT Press: Cambridge, MA, USA, 1985. [Google Scholar]
- EHT-CHD. Environmental Health Trust and the Children’s Health Defense in a US Federal Appeals Court 2020. Available online: https://www.cadc.uscourts.gov/internet/opinions.nsf/FB976465BF00F8BD85258730004EFDF7/$file/20-1025-1910111.pdf (accessed on 19 January 2023).
- ICBE-EMF. Scientific Evidence Invalidates Assumptions Underlying the FCC and ICNIRP Exposure Limits for Radiofrequency Radiation: Implications for 5G. International Commission on the Biological Effects of Electromagnetic Fields (ICBE-EMF). Environ. Health 2022, 21, 92. [Google Scholar] [CrossRef] [PubMed]
- Buchner, K.; Rivasi, M. The International Commission on Non-Ionizing Radiation Protection: Conflicts of Interest, Corporate Interests and the Push for 5G. Brussels. 2020. Available online: https://www.michele-rivasi.eu/wp-content/uploads/2020/06/ICNIRP-report-FINAL-JUNE-2020_EN.pdf (accessed on 19 January 2023).
- Nordhagen, E.K.; Flydal, E. Self-referencing authorships behind the ICNIRP 2020 radiation protection guidelines. Rev. Environ. Health 2022. [Google Scholar] [CrossRef]
- Maisch, D. Notes on the International Conference Mobile Communications and Health: Medical, Biological and Social Problems, Moscow, Russia, 20–22 September 2004. Available online: https://ro.uow.edu.au/cgi/viewcontent.cgi?article=2651&context=artspapers (accessed on 19 January 2023).
- Migliore, A.; Polizzi, N.F.; Therien, M.J.; Beratan, D.N. Biochemistry and Theory of Proton-Coupled Electron Transfer. In Chemical Reviews; Special Issue: Bioinorganic Enzymology; ACS Publications: Washington, DC, USA, 2014. [Google Scholar]
- Belevich, I.; Gorbikova, E.; Belevic, N.P.; Rauhamäki, V.; Wikström, M.; Verkhovsky, M.I. Initiation of the proton pump of cytochrome c oxidase. Proc. Natl. Acad. Sci. USA 2010, 107, 18469–18474. [Google Scholar] [CrossRef] [Green Version]
- WOU. Western Oregon University. Online Chemistry Textbooks. CH450 and CH451: Biochemistry—Defining Life at the Molecular Level, Chapter 6: Enzyme Principles and Biotechnological Applications. 2022. Available online: https://wou.edu/chemistry/courses/online-chemistry-textbooks/ch450-and-ch451-biochemistry-defining-life-at-the-molecular-level/chapter-7-enzyme-kinetics/ (accessed on 19 January 2023).
- AG-EMF. Guideline of the Austrian Medical Association for the Diagnosis and Treatment of EMF Related Health Problems and Illnesses (EMF Syndrome). Consensus Paper of the Austrian Medical Association’s EMF Working Group. 2012. Available online: https://electromagnetichealth.org/wp-content/uploads/2012/04/EMF-Guideline.pdf (accessed on 19 January 2023).
- International Institute for Bau-Biologie & Ecology IBE SBM-2008C. Standard of Building Biology Testing Methods. 2019. Available online: https://buildingbiologyinstitute.org/wp-content/uploads/2019/03/SBM-2008C-v3.6.pdf (accessed on 19 January 2023).
- Dudley, G.B.; Richert, R.; Stiegman, A.E. On the existence of and mechanism for microwave specific reaction rate enhancement. Chem. Sci. 2015, 6, 2144. [Google Scholar] [CrossRef]
- Hardell, L.; Carlberg, M.; Hansson-Mild, K. Use of mobile phones and cordless phones is associated with increased risk for glioma and acoustic neuroma. Pathophysiology 2013, 20, 85–110. [Google Scholar] [CrossRef]
- Hardell, L.; Carlberg, M.; Söderqvist, F.; Hansson-Mild, K. Pooled analysis of case-control studies on acoustic neuroma diagnosed 1997–2003 and 2007–2009 and use of mobile and cordless phones. Int. J. Oncol. 2013, 43, 1036–1044. [Google Scholar] [CrossRef] [Green Version]
- Hardell, L.; Carlberg, M. Mobile phone and cordless phone use and the risk for glioma—Analysis of pooled case-control studies in Sweden, 1997–2003 and 2007–2009. Pathophysiology 2015, 22, 1–13. [Google Scholar] [CrossRef]
- Hardell, L.; Carlberg, M. Increasing rates of brain tumours in the Swedish national inpatient register and the causes of death register. Int. J. Environ. Res. Public Health 2015, 12, 3793–37813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardell, L.; Carlberg, M. Mobile phones, cordless phones and rates of brain tumors in different age groups in the Swedish National Inpatient Register and the Swedish Cancer Register during 1998–2015. PLoS ONE 2017, 12, e0185461. [Google Scholar] [CrossRef] [Green Version]
- Philips, A.; Henshaw, D.L.; Lamburn, G.; O’Carroll, M.J. Brain Tumours: Rise in Glioblastoma Multiforme Incidence in England 1995-2015 Suggests an Adverse Environmental or Lifestyle Factor. J. Environ. Public Health 2018, 2018, 7910754. [Google Scholar]
- Interphone Study Group. Brain tumour risk in relation to mobile telephone use: Results of the Interphone international case-control study. Int. J. Epidemiol. 2010, 39, 675–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Interphone Study Group. Acoustic neuroma risk in relation to mobile telephone use: Results of the Interphone international case-control study. Cancer Epidemiol. 2011, 35, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Coureau, G.; Bouvier, G.; Lebailly, P.; Fabbro-Peray, P.; Gruber, A.; Leffondre, K.; Guillamo, J.S.; Loiseau, H.; Mathoulin-Pelissier, S.; Salamon, R.; et al. Mobile phone use and brain tumours in the CERENAT case-control study. Occup. Environ. Med. 2014, 71, 514–522. [Google Scholar] [CrossRef] [Green Version]
- Belpomme, D.; Hardell, L.; Belyaev, I.; Burgio, E.; Carpenter, D.O. Thermal and non-thermal health effects of low intensity non-ionizing radiation: An international perspective. Environ. Pollut. 2018, 242 Pt A, 643–658. [Google Scholar] [CrossRef]
- de Salles, A.A.; Bulla, G.; Rodriguez, C.E.F. Electromagnetic Absorption in the Head of Adults and Children due to Mobile Phone Operation Close to the Head. Electromagn. Biol. Med. 2006, 25, 349–360. [Google Scholar] [CrossRef]
- Gandhi, O.P.; Morgan, L.L.; de Salles, A.A.; Han, Y.Y.; Herberman, R.B.; Davis, D.L. Exposure limits: The underestimation of absorbed cell phone radiation, especially in children. Electromagn. Biol. Med. 2012, 31, 34–51. [Google Scholar] [CrossRef]
- Fernandez-Rodriguez, C.; de Salles, A.A.; Davis, D.L.; Morgan, L. SAR simulations in SAM varying the dimensions, the distances and the age dependent dielectric parameters. In Proceedings of the 2015 SBMO/IEEE MTT-S International Microwave and Optoelectronics Conference (IMOC), Porto de Galinhas, Brazil, 3–6 November 2015. [Google Scholar] [CrossRef]
- Fernandez-Rodriguez, C.; de Salles, A.A.; Sears, M.E.; Morris, R.D.; Davis, D.L. Absorption of wireless radiation in the child versus adult brain and eye from cell phone conversation or virtual reality. Environ. Res. 2018, 167, 694–699. [Google Scholar] [CrossRef]
- Abecasis, M.; Cross, N.C.P.; Brito, M.; Ferreira, I.; Sakamoto, K.M.; Hijiya, N.; Score, J.; Gale, R.P. Is cancer latency an outdated concept? Lessons from chronic myeloid leukemia. Leukemia 2020, 34, 2279–2284. [Google Scholar] [CrossRef]
- Hardell, L.; Carlberg, M. Comments on the US National Toxicology Program technical reports on toxicology and carcinogenesis study in rats exposed to whole-body radiofrequency radiation at 900 MHz and in mice exposed to whole-body radiofrequency radiation at 1900 MHz. Int. J. Oncol. 2019, 54, 111–127. [Google Scholar] [PubMed] [Green Version]
- Carlberg, M.; Hedendahl, L.; Ahonen, M.; Koppel, T.; Hardell, L. Increasing incidence of thyroid cancer in the Nordic countries with main focus on Swedish data. BMC Cancer 2016, 16, 426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joung, J.Y.; Lim, J.; Oh, C.-M.; Jung, K.-W.; Cho, H.; Kim, S.H.; Seo, H.K.; Park, W.S.; Chung, J.; Lee, K.H.; et al. Risk of Second Primary Cancer among Prostate Cancer Patients in Korea: A Population-Based Cohort Study. PLoS ONE 2015, 10, e0140693. [Google Scholar] [CrossRef] [PubMed]
- Carlberg, M.; Koppel, T.; Hedendahl, L.K.; Hardell, L. Is the Increasing Incidence of thyroid cancer in the Nordic countries caused by use of Mobile Phones? Int. J. Environ. Res. Public Health 2020, 17, 9129. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Deziel, N.C.; Huang, H.; Chen, Y.; Ni, X.; Ma, S.; Udelsman, R.; Zhang, Y. Cell phone use and risk of thyroid cancer: A population-based case-control study in Connecticut. Ann. Epidemiol. 2019, 29, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Li, H.; Deziel, N.C.; Huang, H.; Zhao, N.; Ma, S.; Ni, X.; Udelsman, R.; Zhang, Y. Genetic susceptibility may modify the association between cell phone use and thyroid cancer: A population-based case-control study in Connecticut. Environ. Res. 2020, 182, 109013. [Google Scholar] [CrossRef]
- Choi, Y.J.; Moskowitz, J.M.; Myung, S.K.; Lee, Y.R.; Hong, Y.C. Cellular phone use and risk of tumors: Systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 8079. [Google Scholar] [CrossRef]
- IARC. Report of the Advisory Group to Recommend Priorities for the IARC Monographs during 2020–2024. IARC, World Health Organization 2019. Available online: https://monographs.iarc.fr/wp-content/uploads/2019/10/IARCMonographs-AGReport-Priorities_2020-2024.pdf (accessed on 19 January 2023).
- Chou, C.K.; Guy, A.W.; Kunz, L.L.; Johnson, R.B.; Crowley, J.J.; Krupp, J.H. Long-term, low-level microwave irradiation of rats. Bioelectromagnetics 1992, 13, 469–496. [Google Scholar] [CrossRef]
- Repacholi, M.H.; Basten, A.; Gebski, V.; Noonan, D.; Finnie, J.; Harris, A.W. Lymphomas in E mu-Pim1 transgenic mice exposed to pulsed 900 MHZ electromagnetic fields. Radiat. Res. 1997, 147, 631–640. [Google Scholar] [CrossRef]
- Lerchl, A.; Klose, M.; Grote, K.; Wilhelm, A.F.X.; Spathmann, O.; Fiedler, T.; Streckert, J.; Hansen, V.; Clemens, M. Tumor promotion by exposure to radiofrequency electromagnetic fields below exposure limits for humans. Biochem. Biophys. Res. Commun. 2015, 459, 585–590. [Google Scholar] [CrossRef]
- National Toxicology Program. NTP Technical Report on the Toxicology and Carcinogenesis Studies in B6C3F1/N Mice Exposed to Whole-Body Radio Frequency Radiation at a Frequency (1900 MHz) and Modulations (GSM and CDMA) Used by Cell Phones; NTP TR 596; National Toxicology Program: Research Triangle Park, NC, USA, 2018. Available online: https://www.ncbi.nlm.nih.gov/books/NBK564537/ (accessed on 19 January 2023).
- National Toxicology Program. NTP Technical Report on the Toxicology and Carcinogenesis Studies in Sprague Dawley (Hsd:Sprague Dawley® SD®) Rats Exposed to Whole-body Radio Frequency Radiation at a Frequency (900 Mhz) and Modulations (GSM and CDMA) Used by Cell Phones; NTP TR 595; National Toxicology Program: Research Triangle Park, NC, USA, 2018. Available online: https://www.ncbi.nlm.nih.gov/books/NBK561730/ (accessed on 19 January 2023).
- Li, Y.; Héroux, P. Extra-Low-Frequency Magnetic Fields alter Cancer Cells through Metabolic Restriction. Electromagn. Biol. Med. 2013, 33, 264–275. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Héroux, P. Magnetic Fields Trump Oxygen in Controlling the Death of Erythro-Leukemia Cells. Appl. Sci. 2019, 9, 5318. [Google Scholar] [CrossRef] [Green Version]
- Belpoggi, F. Health impact of 5G. European Parliamentary Research Service Scientific Foresight Unit (STOA) PE 690.012. 2021. Available online: https://www.europarl.europa.eu/RegData/etudes/STUD/2021/690012/EPRS_STU(2021)690012_EN.pdf (accessed on 19 January 2023).
- Herbert, M.R.; Sage, C. Autism and EMF? Plausibility of a pathophysiological link—Part I. Pathophysiology 2013, 20, 191–209. [Google Scholar] [CrossRef] [PubMed]
- Herbert, M.R.; Sage, C. Autism and EMF? Plausibility of a pathophysiological link Part II. Pathophysiology 2013, 20, 211–234. [Google Scholar] [CrossRef]
- Zhang, X.; Huang, W.-J.; Chen, W.-W. Microwaves and Alzheimer’s disease (Review). Exp. Ther. Med. 2016, 12, 1969–1972. [Google Scholar] [CrossRef] [Green Version]
- Carroll, C.M.; Macauley, S.L. The Interaction Between Sleep and Metabolism in Alzheimer’s Disease: Cause or Consequence of Disease? Front. Aging Neurosci. 2019, 11, 258. [Google Scholar] [CrossRef]
- Dasdag, O.; Adalier, N.; Dasdag, S. Electromagnetic radiation and Alzheimer’s disease. Biotechnol. Biotechnol. Equip. 2020, 34, 1087–1094. [Google Scholar] [CrossRef]
- Winklhofer, K.F.; Haass, C. Mitochondrial dysfunction in Parkinson’s disease. Biochim. Et Biophys. Acta 2010, 1802, 29–44. [Google Scholar] [CrossRef]
- Subramaniam, S.R.; Chesselet, M.-F. Mitochondrial dysfunction and oxidative stress in Parkinson’s disease. Prog. Neurobiol. 2013, 106–107, 17–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belpomme, D.; Irigaray, P. Why electrohypersensitivity and related symptoms are caused by non-ionizing man-made electromagnetic fields: An overview and medical assessment. Environ. Res. 2022, 212, 113374. [Google Scholar] [CrossRef]
- International Commission on Non-Ionizing Radiation Protection. General approach to protection against non-ionizing radiation. Health Phys. 2002, 82, 540–548. [Google Scholar] [CrossRef]
- European Economic and Social Committee. Digitalisation—Challenges of Europe. 2019. Available online: https://www.eesc.europa.eu/sites/default/files/files/qe-01-19-295-en-n.pdf (accessed on 19 January 2023).
- The Connexion. French Court Orders 4G Antenna Switch-off over Cow Health Concerns. 2020. Available online: connexionfrance.com/article/French-news/French-court-orders-4G-antenna-switch-off-over-cow-health-concerns (accessed on 19 January 2023).
- Levitt, B.B.; Lai, H.C.; Manville, A.M., II. Effects of non-ionizing electromagnetic fields on flora and fauna, part 1. Rising ambient EMF levels in the environment. Rev. Environ. Health 2021, 37, 81–122. [Google Scholar] [CrossRef] [PubMed]
- Levitt, B.B.; Lai, H.C.; Manville, A.M., II. Effects of non-ionizing electromagnetic fields on flora and fauna, Part 2 impacts: How species interact with natural and man-made EMF. Rev. Environ. Health 2021, 37, 327–406. [Google Scholar] [CrossRef] [PubMed]
- Levitt, B.B.; Lai, H.C.; Manville, A.M., II. Effects of non-ionizing electromagnetic fields on flora and fauna, Part 3. Exposure standards, public policy, laws, and future directions. Rev. Environ. Health 2021, 37, 531–558. [Google Scholar] [CrossRef]
- Hardell, L.; Näsman, A.; Pahlson, A.; Hallquist, A.; Hansson Mild, K. Use of cellular telephones and the risk for brain tumors: A case-control study. Int. J. Oncol. 1999, 15, 113–116. [Google Scholar] [PubMed]
- Volkow, N.D.; Tomasi, D.; Wang, G.-J.; Vaska, P.; Fowler, J.S.; Telang, F.; Alexoff, D.; Logan, J.; Wong, C. Effects of Cell Phone Radiofrequency Signal Exposure on Brain Glucose Metabolism. JAMA 2011, 305, 808. [Google Scholar] [CrossRef] [PubMed]
- Kıvrak, E.G.; Yurt, K.K.; Kaplan, A.A.; Alkan, I.; Altun, G. Effects of electromagnetic fields exposure on the antioxidant defense system. J. Microsc. Ultrastruct. 2017, 5, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Cleveland, R.F., Jr.; Athey, T.W. Specific Absorption Rate (SAR) in models of the human head exposed to hand-held UHF portable radios. Bioelectromagnetics 1989, 10, 173–186. [Google Scholar] [CrossRef] [PubMed]
- Borup, D.T.; Gandhi, O.P. Fast-Fourier-Transform Method for Calculation of SAR Distributions in Finely Discretized Inhomogeneous Models of Biological Bodies. IEEE Trans. Microw. Theory Tech. 1984, 32, 335–360. [Google Scholar] [CrossRef]
- Roe, S. We tested popular cellphones for radiofrequency radiation. Now the FCC is investigating. Chicago Tribune. 2019. Available online: https://www.chicagotribune.com/investigations/ct-cell-phone-radiation-testing-20190821-72qgu4nzlfda5kyuhteiieh4da-story.html (accessed on 19 January 2023).
- Elsheakh, D.; Abdallah, E. Design of low SAR planar monopole antenna for mobile wireless communication applications. Prog. Electromagn. Res. M 2013, 29, 137–149. [Google Scholar] [CrossRef] [Green Version]
- Foster, K.R.; Chou, C.K. Are Children More Exposed to Radio Frequency Energy from Mobile Phones than Adults? IEEE Access 2014, 2, 1497–1509. [Google Scholar] [CrossRef]
- Zonoori, S.I. A comparative study of the distance effects of human head from mobile phone radiation. Int. J. Microw. Opt. Technol. 2015, 10, 20. [Google Scholar]
- Gandhi, O.P. Microwave Emissions From Cell Phones Exceed Safety Limits in Europe and the US When Touching the Body. IEEE Access 2019, 7, 47050–47052. [Google Scholar] [CrossRef]
- Varheenmaa, H.; Lehtovuori, A.; Ylä-Oijala, P.; Viikari, V. Low-SAR Back Cover Mobile Antenna. IEEE Open J. Antennas Propag. 2022, 3, 1154–1160. [Google Scholar] [CrossRef]
- Grant, J.A.; Ragner, G.D.; Geesey, J.G. Inverted Safety Antenna for Personal Communication Device. U.S. Patent 6,741,215 B2, 5 May 2004. Available online: https://patents.google.com/patent/US6741215B2/en (accessed on 19 January 2023).
- Phonegate. Dr. Marc Arazi. 2022. Available online: https://phonegatealert.org/en/ (accessed on 19 January 2023).
- Myung, S.K.; Ju, W.; McDonnell, D.D.; Lee, Y.J.; Kazinets, G.; Cheng, C.-T.; Moskowitz, J.M. Mobile phone use and risk of tumors: A meta-analysis. J. Clin. Oncol. 2009, 27, 5565–5572. [Google Scholar] [CrossRef] [PubMed]
- von Bartheld, C.S.; Bahney, J.; Herculano-Houzel, S. The search for true numbers of neurons and glial cells in the human brain: A review of 150 years of cell counting. J. Comp. Neurol. 2016, 524, 3865–3895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martincorena, I.; Raine, K.M.; Gerstung, M.; Dawson, K.J.; Haase, K.; Van Loo, P.; Davies, H.; Stratton, M.R.; Campbell, P.J. Universal Patterns of Selection in Cancer and Somatic Tissues. Cell 2017, 171, 1029–1041. [Google Scholar] [CrossRef]
- Chrétien, D.; Bénit, P.; Ha, H.-H.; Keipert, S.; El-Khoury, R.; Chang, Y.-T.; Jastroch, M.; Jacobs, H.T.; Rustin, P.; Rak, M. Mitochondria are physiologically maintained at close to 50 °C. PLoS Biol. 2018, 16, e2003992. [Google Scholar] [CrossRef] [Green Version]
- Beignon, F.; Gueguen, N.; Tricoire-Leignel, H.; Mattei, C.; Lenaers, G. The multiple facets of mitochondrial regulations controlling cellular thermogenesis. Cell. Mol. Life Sci. 2022, 79, 525. [Google Scholar] [CrossRef] [PubMed]
- Yeargers, E.K.; Langley, J.B.; Sheppard, A.P.; Huddleston, G.K. Effects of microwave radiation of enzymes. Ann. N. Y. Acad. Sci. 1975, 28, 301–304. [Google Scholar] [CrossRef]
- Sun, W.-C.; Guy, P.M.; Jahngen, J.H.; Rossomando, E.F.; Jahngen, E.G.E. Microwave-Induced Hydrolysis of PhosphoAnhydride Bonds in Nucleotide Triphosphates. J. Org. Chem. 1988, 53, 4414–4416. [Google Scholar] [CrossRef]
- Dayal, B.; Ertel, N.H. Rapid Hydrolysis of Bile Acid Conjugates Using Microwaves: Retention of Absolute Stereochemistry in the Hydrolysis of (25R) 3α,7α,12α-Trihydroxy-5β-cholestan-26-oyltaurine. Lipids 1998, 33, 333. [Google Scholar] [CrossRef]
- Rosana, M.R.; Tao, Y.; Stiegman, A.E.; Dudley, G.B. On the rational design of microwave-actuated organic reactions. Chem. Sci. 2012, 3, 1240–1244. [Google Scholar] [CrossRef]
- Dreyfuss, M.S.; Chipley, J.R. Comparison of Effects of Sublethal Microwave Radiation and Conventional Heating on the Metabolic Activity of Staphylococcus aureus. Appl. Environ. Microbiol. 1980, 39, 13–16. [Google Scholar] [CrossRef] [Green Version]
- Banik, S.; Bandyopadhyay, S.; Ganguly, S. Bioeffects of microwave—A brief review. Bioresour. Technol. 2003, 87, 155–159. [Google Scholar] [CrossRef]
- de la Hoz, A.; Dıaz-Ortiz, A.; Moreno, A. Microwaves in organic synthesis. Thermal and non-thermal microwave effects. Chem. Soc. Rev. 2005, 34, 164–178. [Google Scholar] [CrossRef] [PubMed]
- Federal Communications Commission. FCC 13-39. 29 March 2013. Available online: https://transition.fcc.gov/Daily_Releases/Daily_Business/2013/db0422/FCC-13-39A1.pdf (accessed on 19 January 2023).
- Akdag, M.; Dasdag, S.; Canturk, F.; Akdag, M.Z. Exposure to non-ionizing electromagnetic fields emitted from mobile phones induced DNA damage in human ear canal hair follicle cells. Electromagn. Biol. Med. 2018, 37, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Kolata, G. A Conversation with: Eleanor R. Adair; Tuning In to the Microwave Frequency. NY Times. 2001. Available online: https://www.nytimes.com/2001/01/16/health/a-conversation-with-eleanor-r-adair-tuning-in-to-the-microwave-frequency.html (accessed on 19 January 2023).
- WHO. The Global Health Observatory. Electromagnetic Fields. 2020. Available online: https://www.who.int/data/gho/data/themes/topics/topic-details/GHO/electromagnetic-fields (accessed on 19 January 2023).
- Blumenthal, R. “Flying Blind” on the Health Effects of 5G Wireless Technology Confirmed at US Senate Hearing After Senator Blumenthal Questions Industry. 2019. Available online: https://ehtrust.org/health-effects-of-5g-wireless-technology-confirmed-at-us-senate-hearing-after-senator-blumenthal-questions-industry/ (accessed on 19 January 2023).
- Hardell, L. World Health Organization, radiofrequency radiation and health—A hard nut to crack (Review). Int. J. Oncol. 2017, 51, 405–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schüz, J.; Pirie, K.; Reeves, G.K.; Floud, S.; Beral, V. Response to Moskowitz and Birnbaum, Taylor, Baldwin; et al. J. Natl. Cancer Inst. 2022, 114, 1555–1556. [Google Scholar] [CrossRef]
- New Hampshire. Final Report of the Commission to Study the Environmental and Health Effects of Evolving 5G Technology; State of New Hampshire: Concord, NH, USA, 2019; Volume 15, pp. 107–110. Available online: https://www.gencourt.state.nh.us/statstudcomm/committees/1474/reports/5G%20final%20report.pdf (accessed on 19 January 2023).
- India Ministry of Communications. Stringent Mobile Radiation Standards Come into Force 2012. Available online: https://www.pib.gov.in/newsite/printrelease.aspx?relid=87152 (accessed on 19 January 2023).
- National Safety Council. Technology Can Reduce Cell Phone Distracted Driving 2022. Available online: https://www.nsc.org/road-safety/safety-topics/distracted-driving/technology-solutions (accessed on 19 January 2023).
- Bankrate. Texting and Driving Statistics 2022. Available online: https://www.bankrate.com/insurance/car/texting-and-driving-statistics/ (accessed on 19 January 2023).
- Gregson, R. Manufacturers Own Patents to Cut Radiation 2001. Available online: https://www.rcrwireless.com/20010604/archived-articles/manufacturers-own-patents-to-cut-radiation (accessed on 19 January 2023).
- Fernández-Rodríguez, C.; Bulla, G.; Soares, N.; Fulgêncio, G.; de Salles, A.A. Review of Low SAR Antennas for Mobile Applications. In Proceedings of the 2021 15th European Conference on Antennas and Propagation (EuCAP), Dusseldorf, Germany, 22–26 March 2021; pp. 1–5. [Google Scholar] [CrossRef]
- Yang, F.; Rahmat-Samii, Y. Electromagnetic Band Gap Structures in Antenna Engineering; Cambridge University Press: Cambridge, UK, 2009; Available online: https://www.cambridge.org/us/academic/subjects/engineering/rf-and-microwave-engineering/electromagnetic-band-gap-structures-antenna-engineering?format=HB&isbn=9780521889919 (accessed on 19 January 2023).
- Mudita Pure. Low SAR Phone. 2022. Available online: https://mudita.com/products/phones/mudita-pure/specs/ (accessed on 19 January 2023).
- ZTE Blade. Low SAR Phone. 2022. Available online: https://www.devicespecifications.com/en/model-sar/f4c64f9c (accessed on 19 January 2023).
- Gerasenko, S.; Joshi, A.; Rayaprolu, S.; Ponnavaikko, K.; Agrawal, D.P. Beacon signals: What, why, how, and where? Computer 2001, 34, 108–110. [Google Scholar] [CrossRef]
- Cellraid. Real-Time RFR Dose Monitor for Cellular Phones. Available online: http://www.cellraid.com/ (accessed on 19 January 2023).
- FOSA. Fiber Optic Sensing Association. 2022. Available online: https://fiberopticsensing.org/ (accessed on 19 January 2023).
- FBA. Fiber Broadband Association. 2022. Available online: https://fiberbroadband.org/ (accessed on 19 January 2023).
- Moskowitz, J.M. Cell Phone Radiation Label Bill Passes Maine Legislature Before Dying, 2014. Press Release Distribution. Available online: https://www.prlog.org/12299052-cell-phone-radiation-label-bill-passes-maine-legislature-before-dying.html (accessed on 19 January 2023).
- Egelko, B. Cell Phone Industry Sues Berkeley over Warning-Labels Law. The Daily 2015. Available online: https://www.sfgate.com/bayarea/article/Cell-phone-industry-sues-Berkeley-over-6314832.php (accessed on 19 January 2023).







| Brand | Cell Phone Model | Separation Distance from the Body in mm |
|---|---|---|
| Apple iPhone | 11, 12, 13, SE, X, XR, XS | 5 |
| Huawei | Y6P | 15 |
| LG | G2 | 10 |
| LG | G3 | 15 |
| Motorola | razr | 25 |
| Nokia | 8110 4G | 15 |
| Samsung | Galaxy S5 | 15 |
| Samsung | Galaxy Note 3 | 10 |
| Samsung | Galaxy Z Fold3 5G | 15 |
| Xiaomi | 12X | 5 |
| Cell Type | Average Volume (µm3) | Average Weight (ng) |
|---|---|---|
| Sperm cell | 30 | 0.030 |
| Red blood cell | 100 | 0.1 |
| Lymphocyte | 130 | 0.13 |
| Neutrophil | 300 | 0.3 |
| Beta cell | 1000 | 1 |
| Enterocyte | 1400 | 1.4 |
| Fibroblast | 2000 | 2 |
| HeLa, cervix | 3000 | 3 |
| Hair cell (ear) | 4000 | 4 |
| Osteoblast | 4000 | 4 |
| Alveolar Macrophage | 5000 | 5 |
| Cardiomyocyte | 15,000 | 15 |
| Megakaryocyte | 30,000 | 30 |
| Fat cell | 600,000 (0.0006 µL) | 600 |
| Oocyte | 4,000,000 (0.004 µL) | 4000 |
| IEEE-ICNIRP 1 or 10 g | 1,000,000,000,000 to 10,000,000,000,000 | 1 or 10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Héroux, P.; Belyaev, I.; Chamberlin, K.; Dasdag, S.; De Salles, A.A.A.; Rodriguez, C.E.F.; Hardell, L.; Kelley, E.; Kesari, K.K.; Mallery-Blythe, E.; et al. Cell Phone Radiation Exposure Limits and Engineering Solutions. Int. J. Environ. Res. Public Health 2023, 20, 5398. https://doi.org/10.3390/ijerph20075398
Héroux P, Belyaev I, Chamberlin K, Dasdag S, De Salles AAA, Rodriguez CEF, Hardell L, Kelley E, Kesari KK, Mallery-Blythe E, et al. Cell Phone Radiation Exposure Limits and Engineering Solutions. International Journal of Environmental Research and Public Health. 2023; 20(7):5398. https://doi.org/10.3390/ijerph20075398
Chicago/Turabian StyleHéroux, Paul, Igor Belyaev, Kent Chamberlin, Suleyman Dasdag, Alvaro Augusto Almeida De Salles, Claudio Enrique Fernandez Rodriguez, Lennart Hardell, Elizabeth Kelley, Kavindra Kumar Kesari, Erica Mallery-Blythe, and et al. 2023. "Cell Phone Radiation Exposure Limits and Engineering Solutions" International Journal of Environmental Research and Public Health 20, no. 7: 5398. https://doi.org/10.3390/ijerph20075398