
Comparative Assessment of Fecal Contamination in Piped-to-Plot Communal Source and Point-of-Drinking Water

 , ,
, ,
Abstract
:1. Introduction
2. Methods and Materials
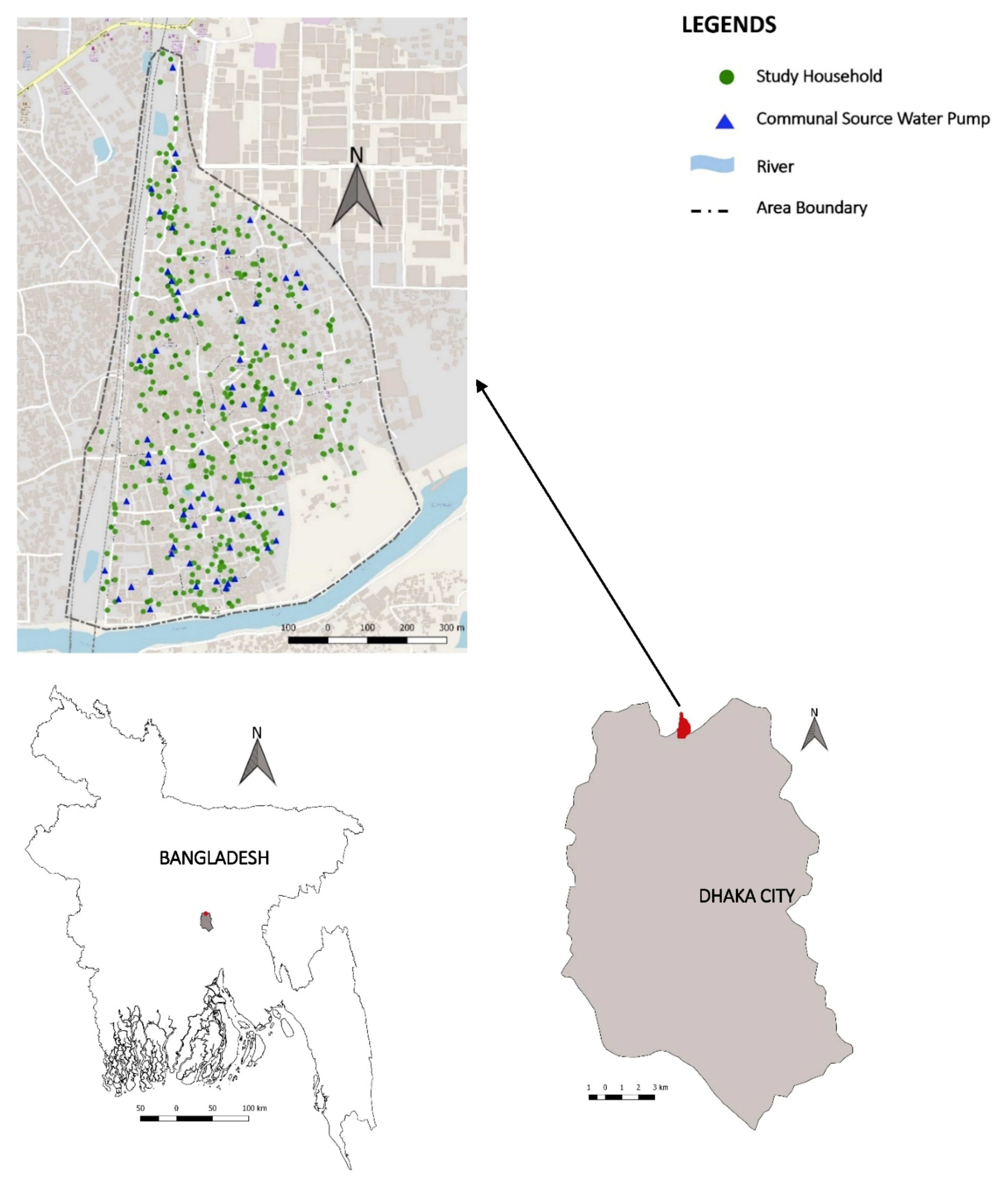
2.1. Study Site and Population
2.2. Types of Water Sources in Arichpur
2.3. Data Collection
2.4. Microbiological Procedures for Sample Collection and Sample Processing
2.5. Data Analysis
3. Results
3.1. Water Quality Assessment by Same-Day Paired Data
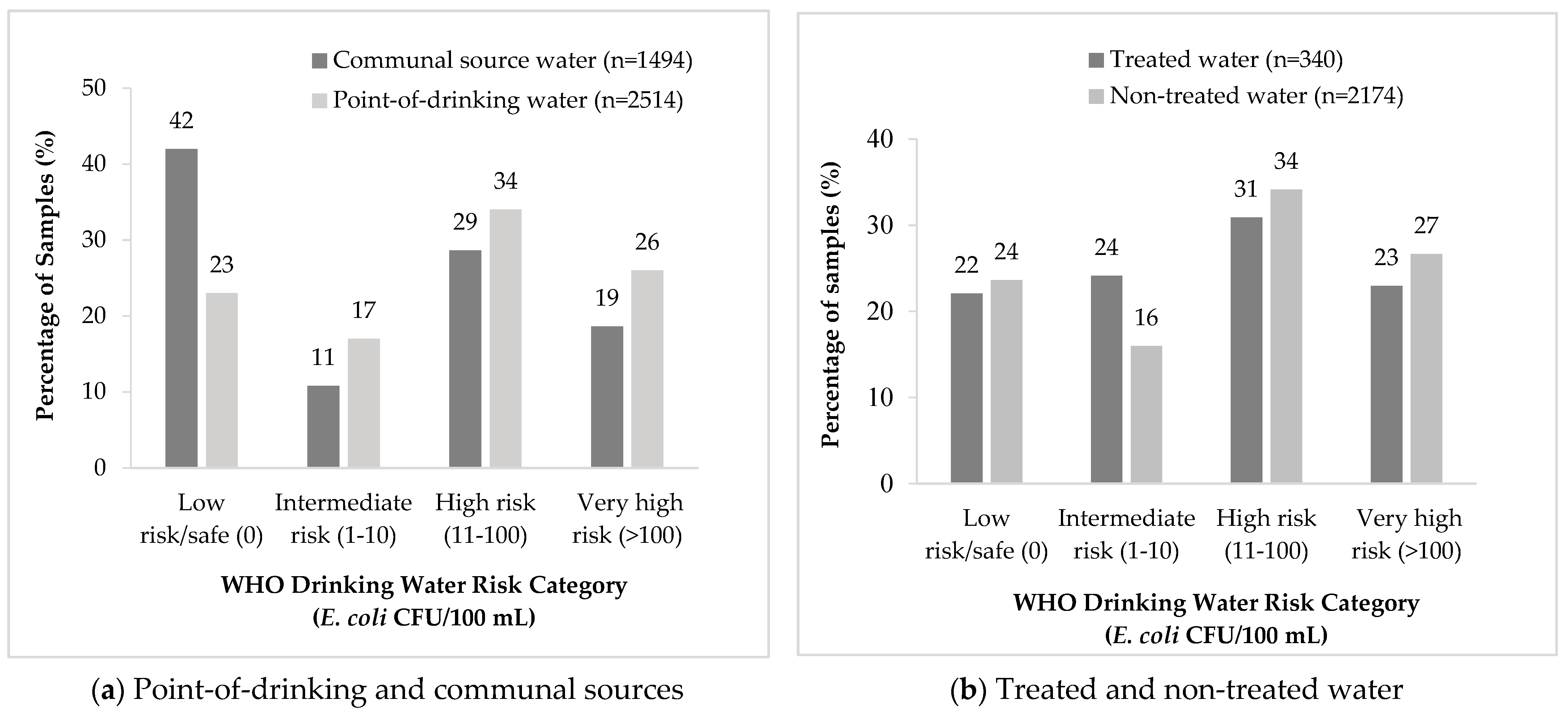
3.2. Water Quality Assessment by WHO Risk Categories
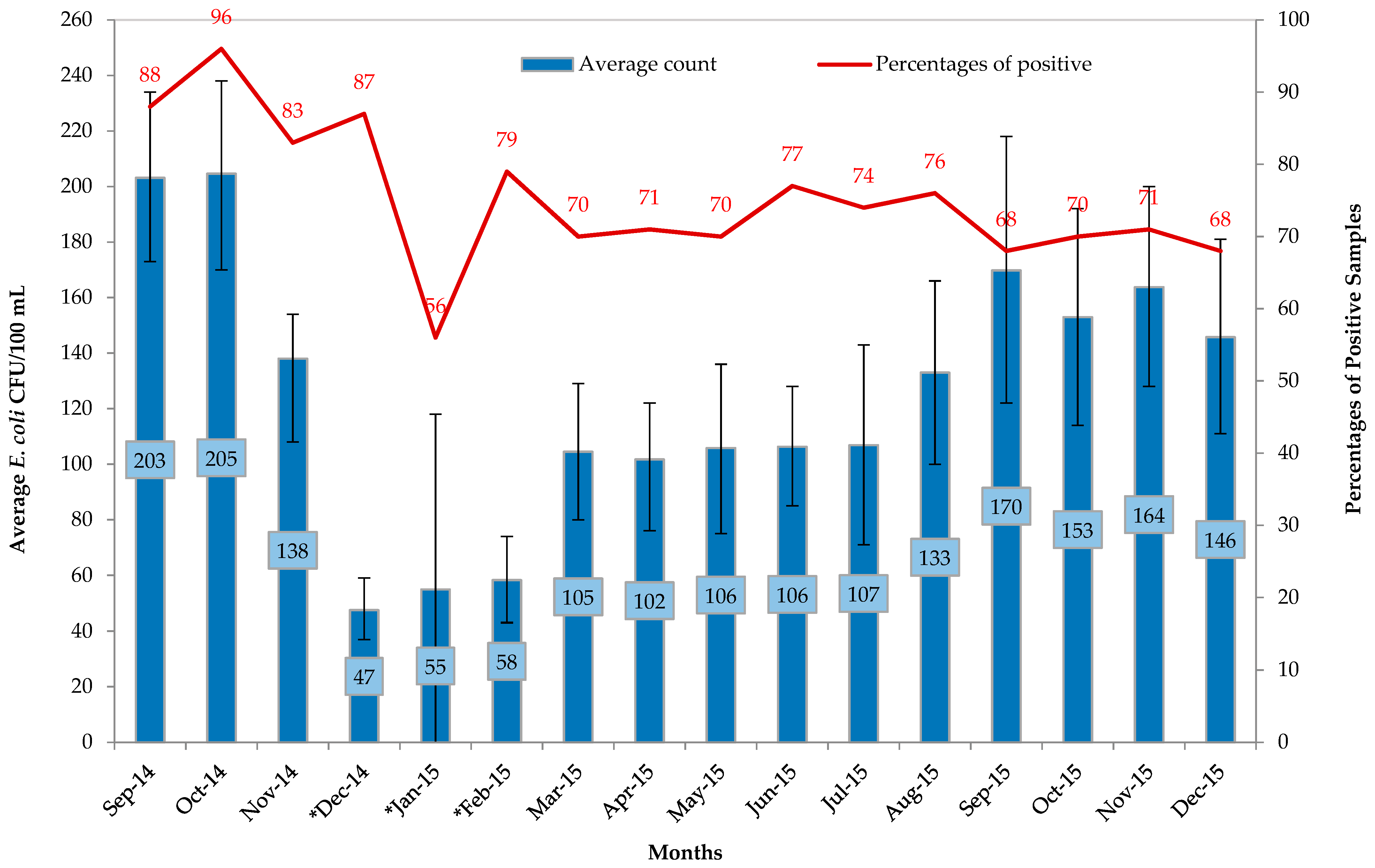
3.3. Temporal Variability of E. coli
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Murray, C.J.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Bain, R.; Cronk, R.; Hossain, R.; Bonjour, S.; Onda, K.; Wright, J.; Yang, H.; Slaymaker, T.; Hunter, P.; Pruss-Ustun, A.; et al. Global assessment of exposure to faecal contamination through drinking water based on a systematic review. Trop. Med. Int. Health 2014, 19, 917–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UNICEF. Progress on Drinking Water, Sanitation and Hygiene. Available online: https://www.unicef.org/publications/files/Progress_on_Drinking_Water_Sanitation_and_Hygiene_2017.pdf (accessed on 12 June 2020).
- WHO; Unicef. Progress on Drinking Water Sanitation and Hygiene: 2017 Update and SDG Baselines. Available online: https://www.who.int/mediacentre/news/releases/2017/launch-version-report-jmp-water-sanitation-hygiene.pdf (accessed on 10 December 2020).
- World Health Organization. Safely Managed Drinking Water: Thematic Report on Drinking Water 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/325897/9789241565424-eng.pdf (accessed on 28 December 2020).
- WHO. Guidelines for Drinking-Water Quality. Available online: http://www.who.int/water_sanitation_health/publications/2011/9789241548151_toc.pdf (accessed on 14 January 2020).
- Bangladesh Bureau of Statistics. Progotir Pathey Bangladesh, Multiple Indicator Cluster Survey. 2019. Available online: https://www.unicef.org/bangladesh/en/reports/progotir-pathey-bangladesh (accessed on 17 February 2020).
- Hoque, B.A.; Hallman, K.; Levy, J.; Bouis, H.; Ali, N.; Khan, F.; Khanam, S.; Kabir, M.; Hossain, S.; Alam, M.S. Rural drinking water at supply and household levels: Quality and management. Int. J. Hyg. Environ. Health 2006, 209, 451–460. [Google Scholar] [CrossRef]
- Wardrop, N.A.; Hill, A.G.; Dzodzomenyo, M.; Aryeetey, G.; Wright, J.A. Livestock ownership and microbial contamination of drinking-water: Evidence from nationally representative household surveys in Ghana, Nepal and Bangladesh. Int. J. Hyg. Environ. Health 2018, 221, 33–40. [Google Scholar] [CrossRef]
- Talukdar, P.K.; Rahman, M.; Rahman, M.; Nabi, A.; Islam, Z.; Hoque, M.M.; Endtz, H.P.; Islam, M.A. Antimicrobial resistance, virulence factors and genetic diversity of Escherichia coli isolates from household water supply in Dhaka, Bangladesh. PLoS ONE 2013, 8, e61090. [Google Scholar] [CrossRef] [Green Version]
- Gakidou, E.; Afshin, A.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulle, A.M.; Abera, S.F.; Aboyans, V. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef] [Green Version]
- Sustainable Development Goals-Goal 11: Sustainable Cities and Communities. Available online: https://www.undp.org/content/undp/en/home/sustainable-development-goals/goal-11-sustainable-cities-and-communities.html (accessed on 24 December 2020).
- Trading Economics. Bangladesh-Population Living In Slums. Available online: https://tradingeconomics.com/bangladesh/population-living-in-slums-percent-of-urban-population-wb-data.html (accessed on 17 February 2020).
- Haque, S.S.; Yanez-Pagans, M.; Arias-Granada, Y.; Joseph, G. Water and sanitation in Dhaka slums: Access, quality, and informality in service provision. Water Int. 2020, 45, 791–811. [Google Scholar] [CrossRef]
- Clasen, T.F.; Alexander, K.T.; Sinclair, D.; Boisson, S.; Peletz, R.; Chang, H.H.; Majorin, F.; Cairncross, S. Interventions to improve water quality for preventing diarrhoea. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Han, A.M.; Oo, K.N.; Midorikawa, Y.; Shwe, S. Contamination of drinking water during collection and storage. Trop. Geogr. Med. 1989, 41, 138–140. [Google Scholar]
- Wright, J.; Gundry, S.; Conroy, R. Household drinking water in developing countries: A systematic review of microbiological contamination between source and point-of-use. Trop. Med. Int. Health 2004, 9, 106–117. [Google Scholar] [CrossRef] [Green Version]
- Gundry, S.W.; Wright, J.A.; Conroy, R.; Du Preez, M.; Genthe, B.; Moyo, S.; Mutisi, C.; Ndamba, J.; Potgieter, N. Contamination of drinking water between source and point-of-use in rural households of South Africa and Zimbabwe: Implications for monitoring the Millennium Development Goal for water. Water Pract. Technol. 2006, 1, wpt2006032. [Google Scholar] [CrossRef]
- Azman, A.S.; Lessler, J.; Satter, S.M.; Mckay, M.V.; Khan, A.; Ahmed, D.; Gurley, E.S. Tracking cholera through surveillance of oral rehydration solution sales at pharmacies: Insights from urban Bangladesh. PLoS Negl. Trop. Dis. 2015, 9, e0004230. [Google Scholar] [CrossRef]
- Sultana, R.; Tamason, C.C.; Carstensen, L.S.; Ferdous, J.; Hossain, Z.Z.; Begum, A.; Jensen, P.K.M. Water usage, hygiene and diarrhea in low-income urban communities—A mixed method prospective longitudinal study. MethodsX 2019, 6, 2822–2837. [Google Scholar] [CrossRef]
- Gurley, E.S.; Hossain, M.J.; Paul, R.C.; Sazzad, H.M.; Islam, M.S.; Parveen, S.; Faruque, L.I.; Husain, M.; Ara, K.; Jahan, Y.; et al. Outbreak of hepatitis E in urban Bangladesh resulting in maternal and perinatal mortality. Clin. Infect. Dis. 2014, 59, 658–665. [Google Scholar] [CrossRef] [Green Version]
- Angeles, G.; Lance, P.; Barden-O’Fallon, J.; Islam, N.; Mahbub, A.Q.M.; Nazem, N.I. The 2005 census and mapping of slums in Bangladesh: Design, select results and application. Int. J. Health Geogr. 2009, 8, 32. [Google Scholar] [CrossRef] [Green Version]
- Islam, N. Slums of Urban Bangladesh: Mapping and Census, 2005; United States Agency for International Development: Dhaka, Bangladesh, 2006.
- Carstensen, L.S.; Tamason, C.C.; Sultana, R.; Tulsiani, S.M.; Phelps, M.D.; Gurley, E.S.; Mackie Jensen, P.K. The Cholera Phone: Diarrheal Disease Surveillance by Mobile Phone in Bangladesh. Am. J. Trop. Med. Hyg. 2019, 100, 510–516. [Google Scholar] [CrossRef] [Green Version]
- United States Environmental Protection Agency. Method 1603: Escherichia coli (E. coli) in Water by Membrane Filtration Using Modified membrane-Thermotolerant Escherichia coli Agar (Modified mTEC). Available online: https://www.epa.gov/sites/production/files/2015-08/documents/method_1603_2009.pdf (accessed on 27 August 2020).
- Szumilas, M. Explaining odds ratios. J. Can. Acad. Child Adolesc. Psychiatry 2010, 19, 227. [Google Scholar]
- Ezeh, A.; Oyebode, O.; Satterthwaite, D.; Chen, Y.F.; Ndugwa, R.; Sartori, J.; Mberu, B.; Melendez-Torres, G.J.; Haregu, T.; Watson, S.I.; et al. The history, geography, and sociology of slums and the health problems of people who live in slums. Lancet 2017, 389, 547–558. [Google Scholar] [CrossRef]
- Schmidt, W.-P.; Cairncross, S. Household water treatment in poor populations: Is there enough evidence for scaling up now? Environ. Sci. Technol. 2009, 43, 986–992. [Google Scholar] [CrossRef]
- Cairncross, S.; Blumenthal, U.; Kolsky, P.; Moraes, L.; Tayeh, A. The public and domestic domains in the transmission of disease. Trop. Med. Int. Health 1996, 1, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Roberts, L.; Chartier, Y.; Chartier, O.; Malenga, G.; Toole, M.; Rodka, H. Keeping clean water clean in a Malawi refugee camp: A randomized intervention trial. Bull. World Health Organ. 2001, 79, 280–287. [Google Scholar]
- Heitzinger, K.; Rocha, C.A.; Quick, R.E.; Montano, S.M.; Tilley, D.H., Jr.; Mock, C.N.; Carrasco, A.J.; Cabrera, R.M.; Hawes, S.E. “Improved” But Not Necessarily Safe: An Assessment of Fecal Contamination of Household Drinking Water in Rural Peru. Am. J. Trop. Med. Hyg. 2015, 93, 501–508. [Google Scholar] [CrossRef] [Green Version]
- Khalil, K.; Lindblom, G.-B.; Mazhar, K.; Kaijser, B. Flies and water as reservoirs for bacterial enteropathogens in urban and rural areas in and around Lahore, Pakistan. Epidemiol. Infect. 1994, 113, 435–444. [Google Scholar] [CrossRef] [Green Version]
- Oswald, W.E.; Lescano, A.G.; Bern, C.; Calderon, M.M.; Cabrera, L.; Gilman, R.H. Fecal contamination of drinking water within peri-urban households, Lima, Peru. Am. J. Trop. Med. Hyg. 2007, 77, 699–704. [Google Scholar] [CrossRef] [Green Version]
- Lindeberg, Y.L.; Egedal, K.; Hossain, Z.Z.; Phelps, M.; Tulsiani, S.; Farhana, I.; Begum, A.; Jensen, P.K.M. Can Escherichia coli fly? The role of flies as transmitters of E. coli to food in an urban slum in Bangladesh. Trop. Med. Int. Health 2018, 23, 2–9. [Google Scholar] [CrossRef] [Green Version]
- Black, R.E.; Lopez de Roma, G.O.; Brown, K.H.; Bravo, N.; Grados Bazalar, O.; Creed Kanashtro, H. Incidence and etiology of infantile diarrhea and major routes of transmission in Huascar, Peru. Am. J. Epidemiol. 1989, 129, 785–799. [Google Scholar] [CrossRef] [Green Version]
- Gil, A.I.; Lanata, C.F.; Hartinger, S.M.; Mäusezahl, D.; Padilla, B.; Ochoa, T.J.; Lozada, M.; Pineda, I.; Verastegui, H. Fecal contamination of food, water, hands, and kitchen utensils at the household level in rural areas of Peru. J. Environ. Health 2014, 76, 102–107. [Google Scholar]
- Sinclair, R.; Gerba, C. Microbial contamination in kitchens and bathrooms of rural Cambodian village households. Lett. Appl. Microbiol. 2011, 52, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Capone, D.; Adriano, Z.; Berendes, D.; Cumming, O.; Dreibelbis, R.; Holcomb, D.A.; Knee, J.; Ross, I.; Brown, J. A localized sanitation status index as a proxy for fecal contamination in urban Maputo, Mozambique. PLoS ONE 2019, 14, e0224333. [Google Scholar] [CrossRef]
- Flores, G.E.; Bates, S.T.; Caporaso, J.G.; Lauber, C.L.; Leff, J.W.; Knight, R.; Fierer, N. Diversity, distribution and sources of bacteria in residential kitchens. Environ. Microbiol. 2013, 15, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Trevett, A.F.; Carter, R.C.; Tyrrel, S.F. The importance of domestic water quality management in the context of faecal–oral disease transmission. J. Water Health 2005, 3, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Zanuzdana, A.; Burkart, K.; Krämer, A. Determinants of diarrhoea in ‘Urban’slums of dhaka and adjacent rural areas: A household-level analysis. Popul. Space Place 2014, 20, 498–511. [Google Scholar] [CrossRef]
- Alam, M.; Islam, A.; Bhuiyan, N.; Rahim, N.; Hossain, A.; Khan, G.Y.; Ahmed, D.; Watanabe, H.; Izumiya, H.; Faruque, A.G. Clonal transmission, dual peak, and off-season cholera in Bangladesh. Infect. Ecol. Epidemiol. 2011, 1, 7273. [Google Scholar] [CrossRef] [Green Version]
- Jensen, P.K.; Ensink, J.H.; Jayasinghe, G.; van der Hoek, W.; Cairncross, S.; Dalsgaard, A. Domestic transmission routes of pathogens: The problem of in-house contamination of drinking water during storage in developing countries. Trop. Med. Int. Health 2002, 7, 604–609. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. of Samples | Contaminated with E. coli, n (%) |
|---|---|---|
| Point-of-drinking water | 2514 | 1926 (77) |
| Water treatment | ||
| Yes | 340 | 265 (78) |
| No | 2174 | 1661 (76) |
| Modes of water treatment * | ||
| Boiling | 254 | 197 (78) |
| Filtration | 83 | 65 (78) |
| Types of drinking vessels * | ||
| Mugs | 1335 | 1035 (78) |
| Glasses | 726 | 568 (78) |
| Bottles | 344 | 232 (67) |
| Jugs | 74 | 62 (84) |
| Communal source water | 1494 | 866 (58) |
| Types of communal water sources | ||
| WASA pump | 122 | 73 (60) |
| Submersible pump | 1372 | 793 (58) |
| Collection points | ||
| Taps attached to the communal pumps | 440 | 208 (47) |
| Taps attached to the reservoir connected to the pumps | 1054 | 658 (62) |
| Difference in E. coli CFU/100 mL between Communal Source and Point-of-Drinking Water | Total No. of Samples (n = 1236) | Mean Changes |
|---|---|---|
| n (%) | ||
| No net change (point-of-drinking = communal source) | 204 (16) | |
| In-house contamination (point-of-drinking > communal source) | 626 (51) | 125 |
| In-house contamination: Ranging low to very high | 314 (26) | 108 |
| Low risk (0) → Intermediate risk (1–10) | 66 (11) | 5 |
| Low risk (0) → High risk (11–100) | 156 (25) | 39 |
| Low risk (0) → Very high risk (>100) | 92 (15) | 300 |
| In-house contamination: Ranging intermediate to very high | 170 (14) | 188 |
| Intermediate risk (1–10) → High risk (11–100) | 34 (5) | 33 |
| Intermediate risk (1–10) → Very high risk (>100) | 36 (6) | 242 |
| High risk (11–100) → Very high risk (>100) | 100 (16) | 221 |
| In-house contamination: no change of risk group | 142 (11) | 85 |
| Intermediate risk (1–10) → Intermediate risk (1–10) | 6 (1) | 4 |
| High risk (11–100) → High risk (11–100) | 75 (12) | 33 |
| Very high risk (>100) → Very high risk (>100) | 61 (10) | 157 |
| Die-off (point-of-drinking < communal source) | 406 (33) | 96 |
| Die-off: Ranging very high to low | 177 (14) | 83 |
| Intermediate risk (1–10) → Low risk (0) | 47 (12) | 6 |
| High risk (11–100) → Low risk (0) | 81 (20) | 37 |
| Very high risk (>100) → Low risk (0) | 49 (12) | 231 |
| Die-off: Ranging very high to intermediate | 124 (10) | 132 |
| High risk (11–100) → Intermediate risk (1–10) | 40 (10) | 29 |
| Very high risk (>100) → Intermediate risk (1–10) | 15 (4) | 276 |
| Very high risk (>100) → High risk (11–100) | 69 (17) | 161 |
| Die off: no change of risk group | 105 (8) | 76 |
| Intermediate risk (1–10) → Intermediate risk (1–10) | 2 (0.5) | 4 |
| High risk (11–100) → High risk (11–100) | 65 (16) | 22 |
| Very high risk (>100) → Very high risk (>100) | 38 (9) | 172 |
| Intermediate Risk (1–10 CFU/100 mL) | High Risk (11–100 CFU/100 mL) | Very High Risk (>100 CFU/100 mL) | |
|---|---|---|---|
| Communal source and point-of-drinking water | |||
| Communal source | n = 161 | n = 428 | n = 278 |
| Median (IQR) | 4 (4, 8) | 32 (20, 56) | 196 (136, 313) |
| Mean (95%CI) | 6 (5, 6) | 40 (38, 43) | 250 (231, 269) |
| Point-of-drinking | n = 428 | n = 844 | n = 655 |
| Median (IQR) | 4 (3, 8) | 36 (20, 62) | 272 (152, 428) |
| Mean (95%CI) | 5 (5, 5) | 42 (41, 44) | 306 (293, 319) |
| Treated and non-treated point-of-drinking water | |||
| Treated | n = 84 | n = 106 | n = 79 |
| Median (IQR) | 4 (2, 6) | 37 (22, 60) | 264 (175, 428) |
| Mean (95% CI) | 4 (4, 5) | 42 (37, 46) | 299 (331, 267) |
| Non-treated | n = 348 | n = 741 | n = 579 |
| Median (IQR) | 4 (3, 8) | 36 (20, 64) | 276 (152, 428) |
| Mean (95% CI) | 5 (5, 5) | 43 (41, 44) | 307 (321, 293) |
| Characteristics | Low Risk/Safe | Intermediate Risk | High Risk | Very High Risk |
|---|---|---|---|---|
| E. coli CFU/100 mL | (<1) | (1–10) | (11–100) | (>100) |
| Treatment | ||||
| Treated, n (%) (n = 340) | 75 (22) | 82 (24) | 105 (31) | 78 (23) |
| OR (CI) | Ref | 1.62 (1.11–2.34) | 0.96 (0.69–1.33) | 0.92 (0.62–1.35) |
| p-value | 0.011 * | 0.824 | 0.660 | |
| Boiling, n (%) (n = 254) | 57 (24) | 68 (27) | 76 (30) | 53 (21) |
| OR (CI) | Ref | 1.61 (0.57–4.55) | 0.87 (0.41–1.84) | 0.73 (0.26–2.08) |
| p-value | 0.361 | 0.722 | 0.565 | |
| Filtration, n (%) (n = 83) | 18 (22) | 14 (17) | 28 (34) | 23 (28) |
| OR (CI) | Ref | 0.66 (0.22–1.95) | 1.17 (0.54–2.53) | 1.37 (0.46–4.06) |
| p-value | 0.458 | 0.687 | 0.568 | |
| Drinking Vessels | ||||
| Mugs, n (%) (n = 1335) | 300 (22) | 214 (16) | 459 (34) | 362 (27) |
| OR (CI) | Ref | 0.96 (0.72–1.26) | 1.14 (0.90–1.44) | 1.19 (0.91–1.54) |
| p-value | 0.773 | 0.251 | 0.191 | |
| Glasses, n (%) (n = 726) | 158 (22) | 129 (18) | 247 (34) | 192 (26) |
| OR (CI) | Ref | 1.17 (0.81–1.68) | 1.12 (0.85–1.48) | 1.12 (0.82–1.54) |
| p-value | 0.387 | 0.412 | 0.454 | |
| Bottles, n (%) (n = 344) | 112 (33) | 56 (16) | 107 (31) | 69 (20) |
| OR (CI) | Ref | 0.63 (0.44–0.92) | 0.62 (0.43–0.87) | 0.50 (0.34–0.73) |
| p-value | 0.019 * | 0.007 * | 0.000 * | |
| Jugs, n (%) (n = 74) | 12 (16) | 18 (24) | 21 (28) | 23 (31) |
| OR (CI) | Ref | 2.10 (0.94–4.70) | 1.22 (0.58–2.59) | 1.75 (0.87–3.52) |
| p-value | 0.069 | 0.591 | 0.114 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferdous, J.; Sultana, R.; Rashid, R.B.; Saima, S.; Begum, A.; Jensen, P.K.M. Comparative Assessment of Fecal Contamination in Piped-to-Plot Communal Source and Point-of-Drinking Water. Water 2021, 13, 1139. https://doi.org/10.3390/w13091139
Ferdous J, Sultana R, Rashid RB, Saima S, Begum A, Jensen PKM. Comparative Assessment of Fecal Contamination in Piped-to-Plot Communal Source and Point-of-Drinking Water. Water. 2021; 13(9):1139. https://doi.org/10.3390/w13091139
Chicago/Turabian StyleFerdous, Jannatul, Rebeca Sultana, Ridwan Bin Rashid, Sabera Saima, Anowara Begum, and Peter Kjær Mackie Jensen. 2021. "Comparative Assessment of Fecal Contamination in Piped-to-Plot Communal Source and Point-of-Drinking Water" Water 13, no. 9: 1139. https://doi.org/10.3390/w13091139