
Detection of SARS-CoV-2 and Variants in Hospital Wastewater in a Developing Country
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection, Handling, and Storage of Wastewater Samples
2.2. Sample Preparation, Concentration, and RNA Extraction
2.3. Recovery Efficiency of the Ultrafiltration Method
2.4. Detection, Verification, and Confirmation of SARS-CoV-2 in Hospital Wastewater Samples
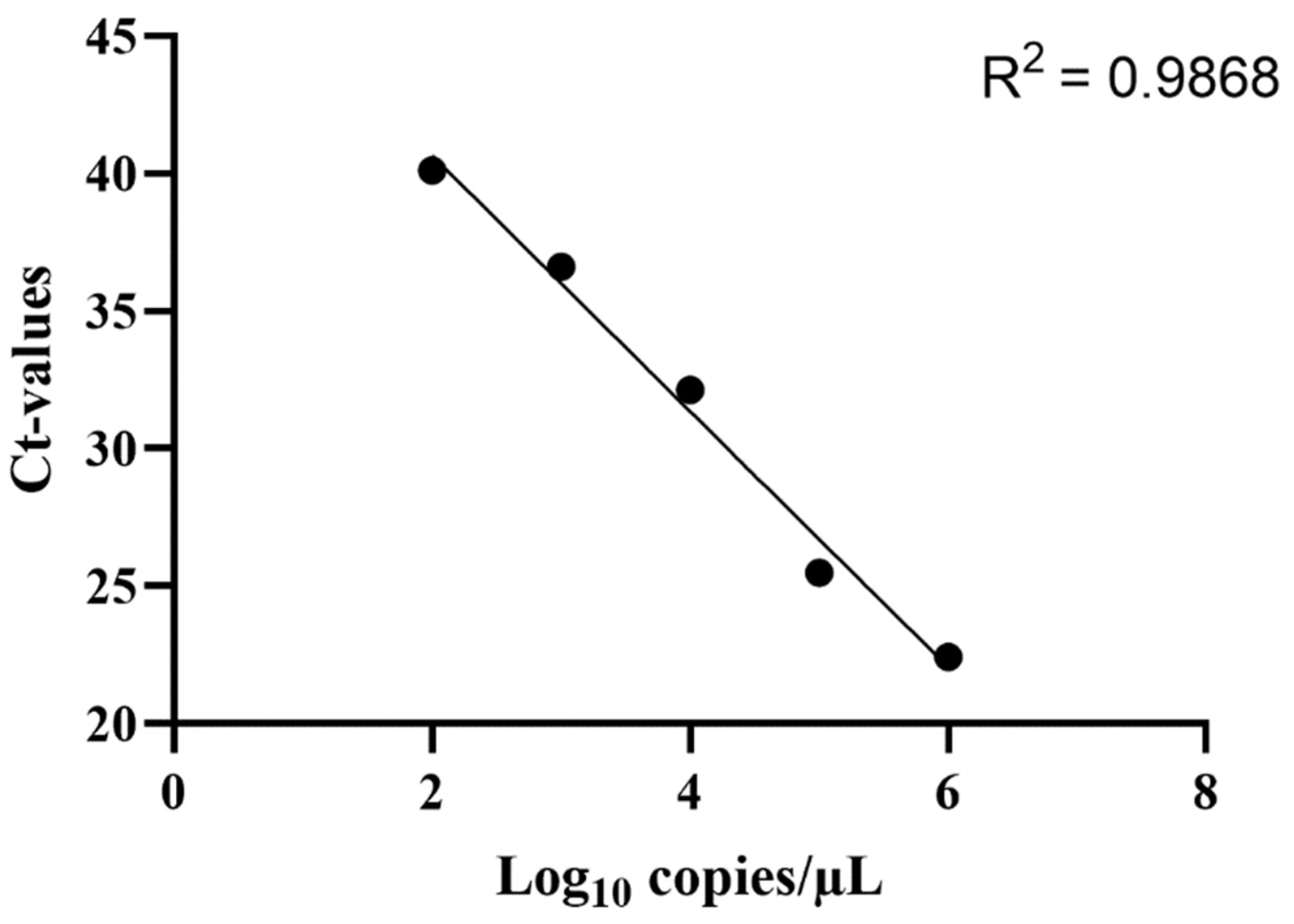
2.5. Quantification of the SARS-CoV-2 RNA Concentration in Hospital Wastewater Samples
2.6. Data Analysis and Cost-Efficiency Analysis
3. Results
3.1. Calculation of Recovery Efficiency of the Ultrafiltration Method
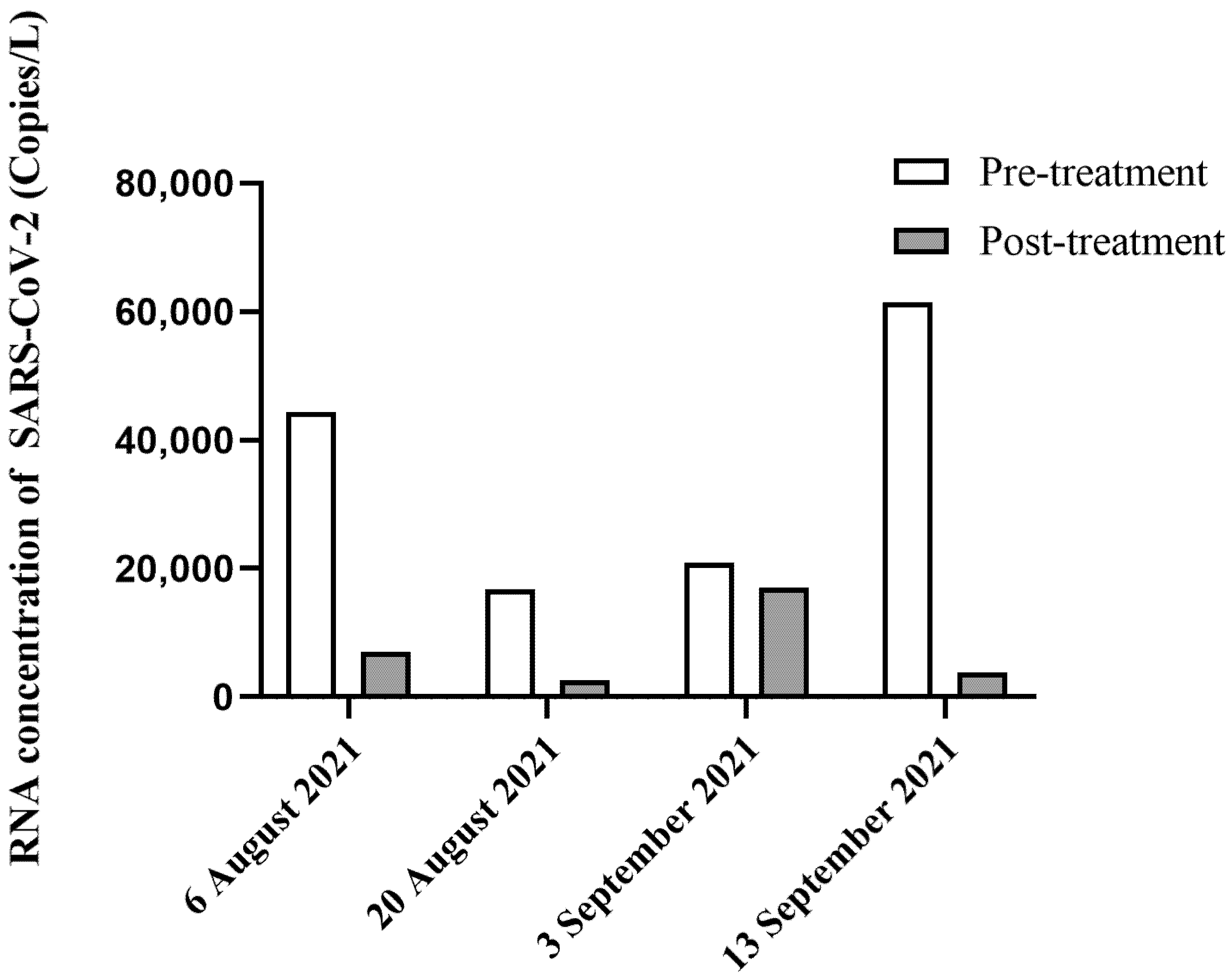
3.2. Detection and Quantification of SARS-CoV-2 RNA in Hospital Wastewater Samples
3.3. Cost-Efficiency Analysis for the Detection of SARS-CoV-2 in Wastewater
3.4. Mutation Sites of the SARS-CoV-2 Partial S Gene in Hospital Wastewater
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harrison, A.G.; Lin, T.; Wang, P. Mechanisms of SARS-CoV-2 Transmission and Pathogenesis. Trends Immunol. 2020, 41, 1100–1115. [Google Scholar] [CrossRef] [PubMed]
- Cevik, M.; Kuppalli, K.; Kindrachuk, J.; Peiris, M. Virology, transmission, and pathogenesis of SARS-CoV-2. BMJ 2020, 371, m3862. [Google Scholar] [CrossRef] [PubMed]
- Kutsuna, S. Clinical Manifestations of Coronavirus Disease 2019. JMA J. 2021, 4, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Islam, M.A.; Kumar, M.; Hossain, M.; Bhattacharya, P.; Islam, M.T.; Hossen, F.; Hossain, M.S.; Islam, M.S.; Uddin, M.M.; et al. First detection of SARS-CoV-2 genetic material in the vicinity of COVID-19 isolation Centre in Bangladesh: Variation along the sewer network. Sci. Total Environ. 2021, 776, 145724. [Google Scholar] [CrossRef]
- Sharif, S.; Ikram, A.; Khurshid, A.; Salman, M.; Mehmood, N.; Arshad, Y.; Ahmed, J.; Safdar, R.M.; Rehman, L.; Mujtaba, G.; et al. Detection of SARs-CoV-2 in wastewater using the existing environmental surveillance network: A potential supplementary system for monitoring COVID-19 transmission. PLoS ONE 2021, 16, e0249568. [Google Scholar] [CrossRef]
- Freire-Paspuel, B.; Garcia-Bereguiain, M.A. Clinical Performance and Analytical Sensitivity of Three SARS-CoV-2 Nucleic Acid Diagnostic Tests. Am. J. Trop. Med. Hyg. 2021, 104, 1516–1518. [Google Scholar] [CrossRef]
- Ahmed, W.; Angel, N.; Edson, J.; Bibby, K.; Bivins, A.; O’Brien, J.W.; Choi, P.M.; Kitajima, M.; Simpson, S.L.; Li, J.; et al. First confirmed detection of SARS-CoV-2 in untreated wastewater in Australia: A proof of concept for the wastewater surveillance of COVID-19 in the community. Sci. Total Environ. 2020, 728, 138764. [Google Scholar] [CrossRef]
- Goncalves, J.; Koritnik, T.; Mioc, V.; Trkov, M.; Boljesic, M.; Berginc, N.; Prosenc, K.; Kotar, T.; Paragi, M. Detection of SARS-CoV-2 RNA in hospital wastewater from a low COVID-19 disease prevalence area. Sci. Total Environ. 2021, 755, 143226. [Google Scholar] [CrossRef]
- Hata, A.; Hara-Yamamura, H.; Meuchi, Y.; Imai, S.; Honda, R. Detection of SARS-CoV-2 in wastewater in Japan during a COVID-19 outbreak. Sci. Total Environ. 2021, 758, 143578. [Google Scholar] [CrossRef]
- Hasan, S.W.; Ibrahim, Y.; Daou, M.; Kannout, H.; Jan, N.; Lopes, A.; Alsafar, H.; Yousef, A.F. Detection and quantification of SARS-CoV-2 RNA in wastewater and treated effluents: Surveillance of COVID-19 epidemic in the United Arab Emirates. Sci. Total Environ. 2021, 764, 142929. [Google Scholar] [CrossRef]
- DDC. COVID-19 Situation in Thailand. Available online: https://ddc.moph.go.th/viralpneumonia/ (accessed on 22 December 2021).
- DDC. COVID-19 Situation in Thailand between April and September. Available online: https://ddc.moph.go.th/viralpneumonia/ (accessed on 22 December 2021).
- Chookajorn, T.; Kochakarn, T.; Wilasang, C.; Kotanan, N.; Modchang, C. Southeast Asia is an emerging hotspot for COVID-19. Nat. Med. 2021, 27, 1495–1496. [Google Scholar] [CrossRef] [PubMed]
- Achak, M.; Alaoui Bakri, S.; Chhiti, Y.; M’Hamdi Alaoui, F.E.; Barka, N.; Boumya, W. SARS-CoV-2 in hospital wastewater during outbreak of COVID-19: A review on detection, survival and disinfection technologies. Sci. Total Environ. 2021, 761, 143192. [Google Scholar] [CrossRef] [PubMed]
- Casanova, L.; Rutala, W.A.; Weber, D.J.; Sobsey, M.D. Survival of surrogate coronaviruses in water. Water Res. 2009, 43, 1893–1898. [Google Scholar] [CrossRef] [PubMed]
- Pham Ngoc Bao, V.D.C. Environmental Resilience and Transformation in Times of COVID-19; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Navarro, A.; Gomez, L.; Sanseverino, I.; Niegowska, M.; Roka, E.; Pedraccini, R.; Vargha, M.; Lettieri, T. SARS-CoV-2 detection in wastewater using multiplex quantitative PCR. Sci. Total Environ. 2021, 797, 148890. [Google Scholar] [CrossRef] [PubMed]
- Anderson-Coughlin, B.L.; Shearer, A.E.H.; Omar, A.N.; Wommack, K.E.; Kniel, K.E. Recovery of SARS-CoV-2 from Wastewater Using Centrifugal Ultrafiltration. Methods Protoc. 2021, 4, 32. [Google Scholar] [CrossRef]
- Fores, E.; Bofill-Mas, S.; Itarte, M.; Martinez-Puchol, S.; Hundesa, A.; Calvo, M.; Borrego, C.M.; Corominas, L.L.; Girones, R.; Rusinol, M. Evaluation of two rapid ultrafiltration-based methods for SARS-CoV-2 concentration from wastewater. Sci. Total Environ. 2021, 768, 144786. [Google Scholar] [CrossRef]
- Fonseca, M.S.; Machado, B.A.S.; Rolo, C.d.A.; Hodel, K.V.S.; Almeida, E.d.S.; de Andrade, J.B. Evaluation of SARS-CoV-2 concentrations in wastewater and river water samples. Case Stud. Chem. Environ. Eng. 2022, 6, 100214. [Google Scholar] [CrossRef]
- Lee, W.L.; Imakaev, M.; Armas, F.; McElroy, K.A.; Gu, X.; Duvallet, C.; Chandra, F.; Chen, H.; Leifels, M.; Mendola, S.; et al. Quantitative SARS-CoV-2 Alpha Variant B.1.1.7 Tracking in Wastewater by Allele-Specific RT-qPCR. Environ. Sci. Technol. Lett. 2021, 8, 675–682. [Google Scholar] [CrossRef]
- Dao, T.L.; Hoang, V.T.; Colson, P.; Lagier, J.C.; Million, M.; Raoult, D.; Levasseur, A.; Gautret, P. SARS-CoV-2 Infectivity and Severity of COVID-19 According to SARS-CoV-2 Variants: Current Evidence. J. Clin. Med. 2021, 10, 2635. [Google Scholar] [CrossRef]
- Li, Q.; Wu, J.; Nie, J.; Zhang, L.; Hao, H.; Liu, S.; Zhao, C.; Zhang, Q.; Liu, H.; Nie, L.; et al. The Impact of Mutations in SARS-CoV-2 Spike on Viral Infectivity and Antigenicity. Cell 2020, 182, 1284–1294.e9. [Google Scholar] [CrossRef]
- Hillary, L.S.; Farkas, K.; Maher, K.H.; Lucaci, A.; Thorpe, J.; Distaso, M.A.; Gaze, W.H.; Paterson, S.; Burke, T.; Connor, T.R.; et al. Monitoring SARS-CoV-2 in municipal wastewater to evaluate the success of lockdown measures for controlling COVID-19 in the UK. Water Res. 2021, 200, 117214. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, W.; Bertsch, P.M.; Bibby, K.; Haramoto, E.; Hewitt, J.; Huygens, F.; Gyawali, P.; Korajkic, A.; Riddell, S.; Sherchan, S.P.; et al. Decay of SARS-CoV-2 and surrogate murine hepatitis virus RNA in untreated wastewater to inform application in wastewater-based epidemiology. Environ. Res. 2020, 191, 110092. [Google Scholar] [CrossRef] [PubMed]
- Wongthida, P.; Liwnaree, B.; Wanasen, N.; Narkpuk, J.; Jongkaewwattana, A. The role of ORF3 accessory protein in replication of cell-adapted porcine epidemic diarrhea virus (PEDV). Arch. Virol. 2017, 162, 2553–2563. [Google Scholar] [CrossRef] [PubMed]
- La Rosa, G.; Mancini, P.; Bonanno Ferraro, G.; Veneri, C.; Iaconelli, M.; Lucentini, L.; Bonadonna, L.; Brusaferro, S.; Brandtner, D.; Fasanella, A.; et al. Rapid screening for SARS-CoV-2 variants of concern in clinical and environmental samples using nested RT-PCR assays targeting key mutations of the spike protein. Water Res. 2021, 197, 117104. [Google Scholar] [CrossRef]
- Ahmed, W.; Bertsch, P.M.; Bivins, A.; Bibby, K.; Farkas, K.; Gathercole, A.; Haramoto, E.; Gyawali, P.; Korajkic, A.; McMinn, B.R.; et al. Comparison of virus concentration methods for the RT-qPCR-based recovery of murine hepatitis virus, a surrogate for SARS-CoV-2 from untreated wastewater. Sci. Total Environ. 2020, 739, 139960. [Google Scholar] [CrossRef]
- Cuevas-Ferrando, E.; Perez-Cataluna, A.; Allende, A.; Guix, S.; Randazzo, W.; Sanchez, G. Recovering coronavirus from large volumes of water. Sci. Total Environ. 2021, 762, 143101. [Google Scholar] [CrossRef]
- Yang, Y.; Xiao, Z.; Ye, K.; He, X.; Sun, B.; Qin, Z.; Yu, J.; Yao, J.; Wu, Q.; Bao, Z.; et al. SARS-CoV-2: Characteristics and current advances in research. Virol. J. 2020, 17, 117. [Google Scholar] [CrossRef]
- Muttineni, R.; Binitha, R.N.; Putty, K.; Marapakala, K.; Sandra, K.P..; Panyam, J.; Vemula, A.; Singh, S.M.; Balachandran, S.; Viroji Rao, S.T.; et al. SARS-CoV-2 variants and spike mutations involved in second wave of COVID-19 pandemic in India. Transbound. Emerg. Dis. 2022, 69, e1721–e1733. [Google Scholar] [CrossRef]
- Jhun, H.; Park, H.Y.; Hisham, Y.; Song, C.S.; Kim, S. SARS-CoV-2 Delta (B.1.617.2) Variant: A Unique T478K Mutation in Receptor Binding Motif (RBM) of Spike Gene. Immune Netw. 2021, 21, e32. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PCR ID | Target Gene | Sequence (5′→3′) | Usage | Size, bp | Ref |
|---|---|---|---|---|---|
| PEDV_M | M gene | 5′ TGTCTACGGACGTGTTGGTC 3′ 5′ AGCTGAGTAGTCGCCGTGTT 3′ | RT-qPCR | 91 | [26] |
| 972 | S | 5′ ACCCTGACAAAGTTTTCAGATCCT 3′ 5′ GCTGAGAGACATATTCAAAAGTGCA 3′ | 1st cycle | 399–408 | [27] |
| 973 | S | 5′ TTCAACTCAGGACTTGTTCTTACC 3′ 5′ TCTGAACTCACTTTCCATCCAA 3′ | Nested | 319–327 |
| Replicates | PEDV Concentration (log10 Copies of PEDV Recovered) | PEDV Copy Numbers per Reaction (5 µL Samples Were Added into Reactions) | % Recovery of PEDV | % Recovery of PEDV (Mean ± SD) |
|---|---|---|---|---|
| 1 | 3.545 | 3.51 × 103 | 53.4 | 80.53 ± 23.526 |
| 2 | 3.794 | 6.23 × 103 | 94.8 | |
| 3 | 3.788 | 6.14 × 103 | 93.4 |
| Procedures | Cost | Cost per Sample | Throughput per Day |
|---|---|---|---|
| Virus concentration | USD 358.98 | USD 14.96 | 48 |
| RNA extraction | USD 131.03 | USD 4.09 | |
| Detection of SARS-CoV-2 | USD 393.10 | USD 16.38 | |
| Total cost | USD 35.43 per sample | ||
| Tracking ID | Mutation Sites | NCBI Blast (Accession Number) |
|---|---|---|
| HW 8719 | H69del, V70del, Y144del | OP022966.1 |
| HW 8723 | G142D | OX243730.1 |
| HW 8765 | G142D | OX243730.1 |
| HW 8778 | - | OX196900.1 |
| HW 8916 | T95I | ON998987.1 |
| HW 8603 | H69del, V70del, Y144del | ON909458.1 |
| HW 9234 | - | OX243720.1 |
| HW 9407 | - | OX243686.1 |
| HW 9473 | - | OX243715.1 |
| HW 9574 | G142D | OX243678.1 |
| HW 9733 | - | ON800253.1 |
| HW 9735 | - | OX243720.1 |
| HW 8602 | H69del, V70del | OX243731.1 |
| HW 8769 | G142D | OX243730.1 |
| HW 8597 | T95I | OP022971.1 |
| HW 9021 | T95I, G142D | OP012924.1 |
| HW 9375 | - | OX243696.1 |
| HW 8777 | - | OX243730.1 |
| HW 8587 | H69del, V70del | OX243731.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tiacharoen, V.; Denpetkul, T.; Kosoltanapiwat, N.; Maneekan, P.; Thippornchai, N.; Saeoueng, A.; Jittmittraphap, A.; Sattabongkot, J.; Leaungwutiwong, P. Detection of SARS-CoV-2 and Variants in Hospital Wastewater in a Developing Country. Water 2022, 14, 3798. https://doi.org/10.3390/w14233798
Tiacharoen V, Denpetkul T, Kosoltanapiwat N, Maneekan P, Thippornchai N, Saeoueng A, Jittmittraphap A, Sattabongkot J, Leaungwutiwong P. Detection of SARS-CoV-2 and Variants in Hospital Wastewater in a Developing Country. Water. 2022; 14(23):3798. https://doi.org/10.3390/w14233798
Chicago/Turabian StyleTiacharoen, Vichapon, Thammanitchpol Denpetkul, Nathamon Kosoltanapiwat, Pannamas Maneekan, Narin Thippornchai, Anon Saeoueng, Akanitt Jittmittraphap, Jetsumon Sattabongkot, and Pornsawan Leaungwutiwong. 2022. "Detection of SARS-CoV-2 and Variants in Hospital Wastewater in a Developing Country" Water 14, no. 23: 3798. https://doi.org/10.3390/w14233798