
Legionella spp. in Thermal Facilities: A Public Health Issue in the One Health Vision

1
Department of Biomedical and Dental Sciences and Morphofunctional Imaging, University of Messina, 98125 Messina, Italy
2
Istituto Polispecialistico C.O.T. Cure Ortopediche Traumatologiche S.p.A., 98124 Messina, Italy
*
Author to whom correspondence should be addressed.
Water 2023, 15(4), 689; https://doi.org/10.3390/w15040689
Submission received: 30 December 2022
/
Revised: 3 February 2023
/
Accepted: 7 February 2023
/
Published: 9 February 2023
(This article belongs to the Section Water and One Health)
Abstract
:Thermal facilities comprise a wide spectrum of recreational and therapeutic activities with the number of customers increasing over time despite the break that occurred during the first phases of the COVID-19 pandemic. In order to evaluate the potential role played by this setting in the risk of contracting legionellosis, we conducted a cross-sectional study to evaluate the presence of Legionella spp. in some Italian thermal facilities. Specifically, we retrospectively analyzed the results of a 16-year surveillance carried out before the COVID-19 pandemic. Of 409 samples, 70 (17.1%) were positive with Legionella spp. but there was an overall decrease over time. L. pneumophila 2–14 were by far the most common detected serotypes, while L. pneumophila 1 accounted for only 8.8%. Of all the different kind of samples, swabs and municipal water samples were the most contaminated. Moreover, in the positive samples, bacterial load was often at intermediate values. In only a small percentage of samples was load high and, in this case, L. pneumophila 1 was often the most common strain. Our results show the importance of a continuous monitoring of Legionella risk in these settings, even more so now after the COVID-19 pandemic and the prolonged break in activities. Water is the natural environment of Legionella spp. and environment in general plays a crucial role in the transmission of these bacteria; therefore, it would be useful to frame this infection in a “One Health” key.
1. Introduction
Legionellosis is caused by inhalation of aerosolized water particles contaminated by waterborne microorganisms belonging to the genus Legionella [1]. This genus is widely distributed in both natural (i.e., rivers, lakes, groundwater, thermal waters) and artificial aquatic environments, such as waterworks of hospitals [2,3,4,5,6,7,8,9], accommodation facilities and private houses [10,11,12,13,14], cooling towers and air conditioners [15], and dental units [16,17,18,19,20]. Theoretically, any water system containing and storing non-sterile water that can be aerosolized is a potential source of Legionella spp.
As water is the natural environment of Legionella spp., and environment in general plays a crucial role in the transmission of these bacteria, it would be necessary to frame this infection in a “One Health” key. “One Health” is a relatively new term, used, according to the World Health Organization (WHO), to indicate “an approach to designing and implementing programs, policies, legislation and research in which multiple sectors communicate and work together to achieve better public health outcomes” [21]. For this reason, a continuous monitoring of the environment is crucial in the infection control. In fact, legionellosis surveillance and containment are current public health targets worldwide, even if the regulatory legislation differs from country to country, despite the presence of common principles such as monitoring critical spots, avoiding water stagnation, and maintaining some water temperature (above 60 °C, below 25 °C) [22].
In 2020, according to the European Centre for Disease Control and Prevention (ECDC), 8372 cases of legionellosis were reported in Europe, of which 7712 (92%) were confirmed [23]. In the same year, according to the last report of the National Higher Health Institute (in Italian ISS), 2074 cases were reported in Italy with a notification rate of 3.8 per 100,000 inhabitants. The incidence of legionellosis was 34.8 cases per million inhabitants with a remarkable decrease compared to the last year (53.0/1,000,000) due to the COVID-19 pandemic [1]. The majority of outbreaks described worldwide are caused by L. pneumophila, in particular serogroup 1, which makes it, therefore, the most common pathogen species for humans; however, other serogroups and species were also associated to human disease, such as L. micdadei, L. dumoffii, and L. longbeachae [24].
Recreational waters can be an important potential route of exposure to legionellosis, especially hot water pools associated with hydromassage systems. According to a recent review analyzing 136 legionellosis outbreaks from 2006 to 2017, of 4367 total confirmed cases with 251 total deaths, 14% of them recognized in recreational waters (pools or spas) an ascertained or suspected source [25]. The role played by this transmission route has acquired even more importance considering the growing attractiveness of private/public recreational facilities and the more and more increasing number of people attending them.
The thermal/mineral springs industry includes a wide variety of different types of facilities, some recreational (e.g., thermal water swimming pools and waterparks), some medical or therapeutic (e.g., many sanatoria in Europe), and some focus on wellness-enhancing experiences (e.g., onsen, thermal springs spas). Many thermal/mineral springs facilities include multiple categories. Thermal therapy comprises a wide spectrum of therapeutic activities including hydrotherapy, balneotherapy, mud-pack therapy, mud-bath therapy, massage, hot showers, supervised water exercises, and inhalatory treatments in spa resorts, which can represent a valid support to pharmacological and/or physiotherapeutic therapies, with positive results on acute and chronic pain, drug use, and patients’ general well-being [26,27]. It can be considered a cost-saving measure in the management of several chronic inflammatory conditions such as rheumatic and respiratory diseases [28,29,30,31,32]. It is estimated that, worldwide, there are about 34,057 thermal/mineral springs facilities operating in 127 countries with a business of $56.2 billion of revenues in 2017, and about 1.8 million workers. The thermal/mineral springs industry is present especially in Asia-Pacific and Europe, together accounting for 95% of industry revenues and 94% of facilities. In Italy, there are 768 thermal/mineral springs facilities with a business of $1718.3 million of revenues in 2017 [33]. In 2014, the number of customers of thermal facilities amounted to 2 million 791 thousand and their average age was further reduced: the proportion of the elderly has fallen to 47%, while the proportion of children up to 17 years of age has risen to 10% and to 43% for adults from 18 to 64 years. With an proportion of 55% of the total, women continue to represent the most significant component of customers [34].
Inside the thermal facilities, the presence of a hot-humid environment favors the growth and spread of microorganisms that have, in such ecosystem, a habitat promoting its colonization [35,36]. Among these microorganisms, Legionella spp. is one of the most common isolated due to its strictly aquatic life cycle, so it is important to put particular attention to this setting through the adoption of control and preventive measures to reduce its spread and, therefore, the risk for customers’ and workers’ health.
The purpose of this research was to analyze the trend of a 16-year surveillance on the presence of Legionella spp. in some Italian thermal/mineral spring facilities in order to evaluate the potential role played by this source in the risk of contracting legionellosis, both for customers and workers.
2. Materials and Methods
This research was carried out by the Regional Reference Laboratory of Clinical and Environmental Surveillance of Legionellosis, section of Messina (Italy), located inside the University Hospital “G. Martino” of Messina, Sicily. Our interest in Legionella started in 1988. At first, it was addressed only to research activities aimed at detecting Legionella spp. in small hospitals, care homes, and other types of structures located in the Messina territory. Since 2004, we have begun to carry out a continuous surveillance at the University Hospital and in 2012, the laboratory was turned into a reference laboratory.
Sicily is a land with a very ancient thermal tradition and, with over 60 thermal springs, rightly represents one of the most important thermal regions in Europe. Unfortunately, despite such a wide hydrological richness, Sicily has just eight operative and efficient thermal/mineral springs facilities and only few types of recognized mineral waters. Of all the working facilities, three are located in the Messina provincial territory (Figure 1) [37].
This paper shows the results of a 16-year surveillance carried out by our laboratory from 2004 to 2019 in samples collected in some of the Sicilian thermal facilities to evaluate the presence of Legionella spp. in different kind of samples. In particular, we collected samples of supplied municipal water, thermal water, swabs swiped on various surfaces in contact with both customers and workers, and, finally, vapors and air/gas mixture. Specifically, four (50%) of the eight working regional thermal facilities were analyzed. All the structures have similar features, being quite old facilities composed of different settings used both for therapy and recreational activities. Moreover, all the studied structures have included hotel facilities to host customers. After 2019, the surveillance was stopped due to the COVID-19 pandemic that caused the total closure of the facilities starting from the begin of 2020 for the general lockdown that was established in Italy.
2.1. Sampling
All the samples were collected at the start of daily activities in accordance with the 2000 [38], and revised 2015 [39], Italian Guidelines for the Prevention and Control of Legionellosis, and were brought to the laboratory as soon as possible and presently processed. In particular, samples of municipal water were collected from taps and showers of living and therapy rooms (mud therapy and pulmonary ventilation rooms), hot and cold water collection tanks, wells, boilers, autoclaves, and entry points of supplied municipal water. For the collection, 1-L sterile glass bottles with 1% sodium thiosulfate to neutralize the presence of chlorine were used. In all the sampled points, water was collected immediately after the opening of the tap without disinfecting or heating the exit point. Moreover, temperature was measured with a precision thermometer (Temp-16 RTD Thermometer, Thermo Fisher Scientific, USA) immersed in the flow of running water. Thermal water samples were collected both directly from the source and from taps, showers and tanks of therapy rooms. Swabs were obtained by rubbing on taps, showers, whirlpool tubs, and aerosol equipment of living and therapy rooms (mud therapy and pulmonary ventilation rooms). Vapors and air/gas mixture were collected form aerosol equipment of therapy rooms using the air sampler Surface Air System 100 (PBI, Milano, Italy).
2.2. Isolation and Serological Identification of Legionella
From water samples, the standard procedures reported by the 2000 Italian Guidelines [38] were adopted; from May 2015 to 2019, the revised 2015 Italian Guidelines [39] were used. In these years, in accordance with the guidelines, 1-L water samples were concentrated to 10 mL through 0.2-μm porosity membrane filters and incubated at 50° C for 30 min in a thermostatic bath. Concentrated and non-concentrated samples were spread in duplicate on plates of Buffered Charcoal-Yeast Extract Agar Base Medium (BCYE Agar, Thermo Fisher Scientific, USA) and incubated for 10 days at 36–37 °C in a moist chamber with 2.5% CO2. The suspected colonies were isolated and confirmed as Legionella spp. after screening their inability to grow on a culture medium without cysteine. Legionella counts were reported in colony forming units/liter (CFUs/L) according to the number of colonies per plate and to the dilutions performed on the original sample. A latex micro-agglutination test kit with polyvalent antisera (Thermo Fisher Scientific, USA) was used to identify the isolates assumed to belong to Legionella spp. For serological identification also “Legionella pneumophila monovalent antisera set 1 and 2” and Legionella antisera for several non-L. pneumophila spp. as L. bozemanii, dumoffii, gormanii, micdadei, etc. (Denka Seiken Co., Ltd., Tokyo, Japan) were used.
Concerning the bacterial load, we divided the isolates into four groups according to the latest national guidelines (point 3.4: “Risk Assessment and Management in the healthcare facilities”) [39]:
- <100 CFUs/L;
- 101–1000 CFUs/L;
- 1001–10,000 CFUs/L;
- 10,001–100,000 CFUs/L.
2.3. Statistical Analysis
All the obtained data were collected and analyzed with Prism 4.0 software. Descriptive statistics were used to find percentages and mean values. The comparison between the groups under study were carried out through correlation tests and chi-square test. Significance was assessed at the p < 0.05 level.
3. Results
From 2004 to 2019, we collected 409 samples of which 123 (30.1%) swabs, 114 (27.9%) samples of municipal water, 77 (18.8%) of thermal water, 65 (15.9%) of vapors, and 30 (7.3%) of air/gas mixture. Concerning the different settings of the surveilled facilities, 67.5% of the samples were collected in therapy rooms (mud therapy rooms, inhalation rooms, and pulmonary ventilation rooms), 25.2% were collected from water storages (tanks and boilers) and 7.3% were collected from customer living rooms.
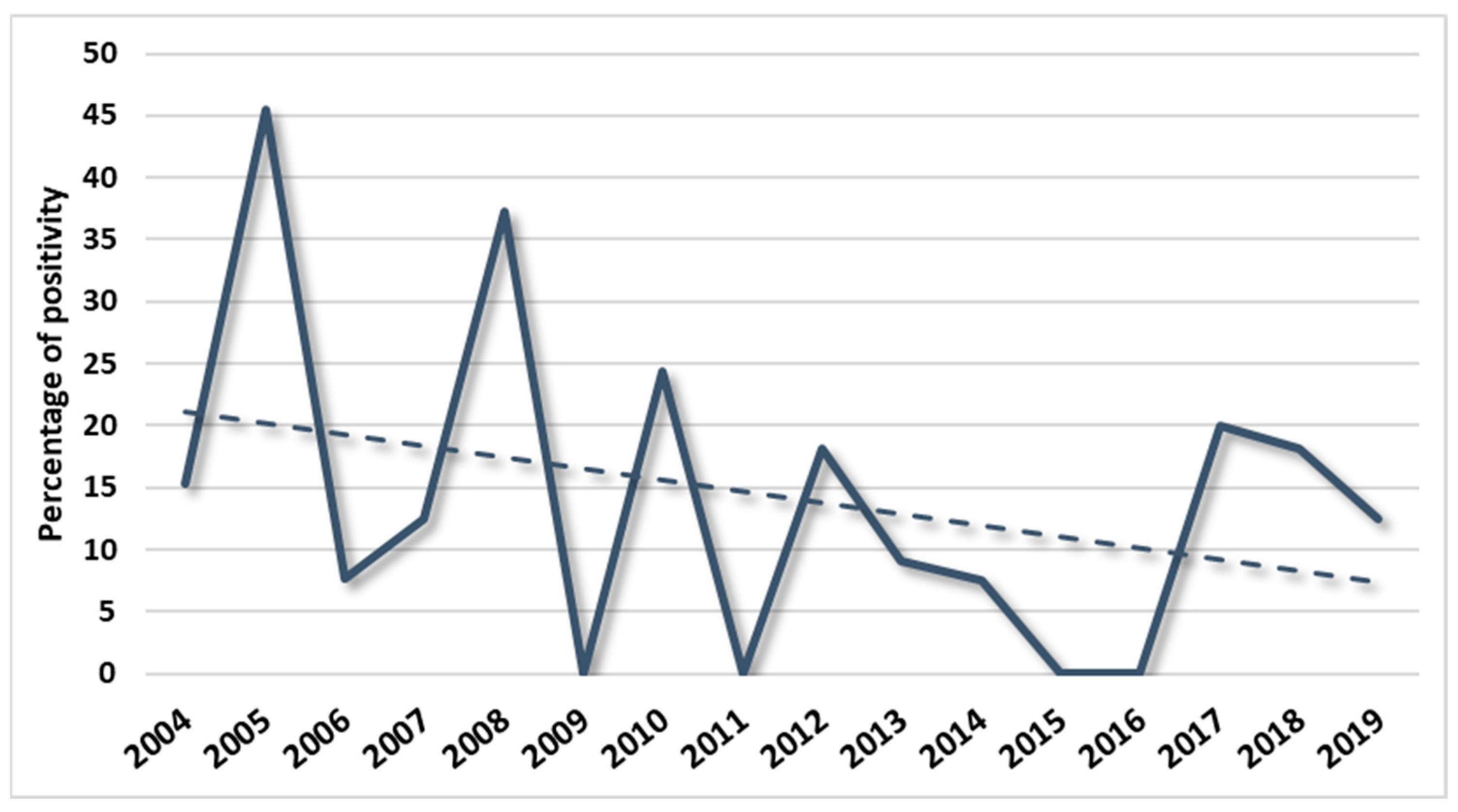
Legionella spp. positive samples was 70 (17.1%), of which 37 (52.8%) were swabs, 17 (24.3%) municipal water samples, 13 (18.6%) thermal water samples, and 3 (4.3%) vapor samples. No air/gas mixture samples were positive to Legionella spp. Table 1 shows the absolute numbers of collected and positive samples with positivity percentage per each year of the surveillance, while Figure 2 shows the graphical representation of the annual temporal trend of the detected Legionella spp. percentage positivity.
The figure shows a very up and down trend with peaks and troughs throughout the surveillance period. Nevertheless, an overall reduction in the positivity was found during the whole surveillance period, even during the recent peaks. Specifically, a statistically significant difference was found between the first half of the surveillance period (2004–2011) and the second half (2012–2019) with positivity percentage of 21.0% and 10.0%, respectively (χ = 4.6192, p = 0.031616). However, a certain increase was found after 2016 with a partial reduction in the last two years of surveillance. In Table 2, the absolute numbers and the positivity percentage of the different kind of samples divided for the places where the same were collected are shown.
The table shows that positive samples were found in many different sections of the facilities. Specifically, of all the 70 positive samples, 71.4% were collected from therapy rooms, 22.9% from water storages, and 5.7% from customer living rooms. Considering that a positivity detected in therapy rooms could be a high risk for customers’ health and play a higher role in the disease transmission compared to other types of settings, we considered two groups according to this different risk class and we evaluated the difference between them. From the statistical analysis, a highly statistically significant difference was found (χ = 35.28; p < 0.00001). Concerning, individually, the different settings, 18.5% of all the samples collected from therapy rooms, 14.6% of those collected from water storages, and 10% of those collected from customers living rooms were positive, without any statistically significant difference among them.
By dividing for typology of samples, concerning swabs, the highest positivity rate was found in those collected from showers and bathtubs of mud therapy rooms and showers and taps of aerosol and inhalation rooms, while considering municipal water, the highest positivity was detected on collection tanks and boilers followed by showers and bathtubs of mud therapy rooms. Moreover, for thermal water samples, the main source of positive samples were collection tanks.
Regarding the isolated strains, L. pneumophila serogroup 1 accounted for only 8.8%, L. pneumophila serogroup 2–14 for 76.8%, and non-L. pneumophila spp. for 17.7%. The total sum is not equal to 100 because 3.3% of the positive samples represented more serogroups at the same time. Specifically, 2.7% was positive for both L. pneumophila serogroup 2–14 and non-L. pneumophila spp. while 0.6% for L. pneumophila serogroup 1 and L. pneumophila serogroup 2–14.
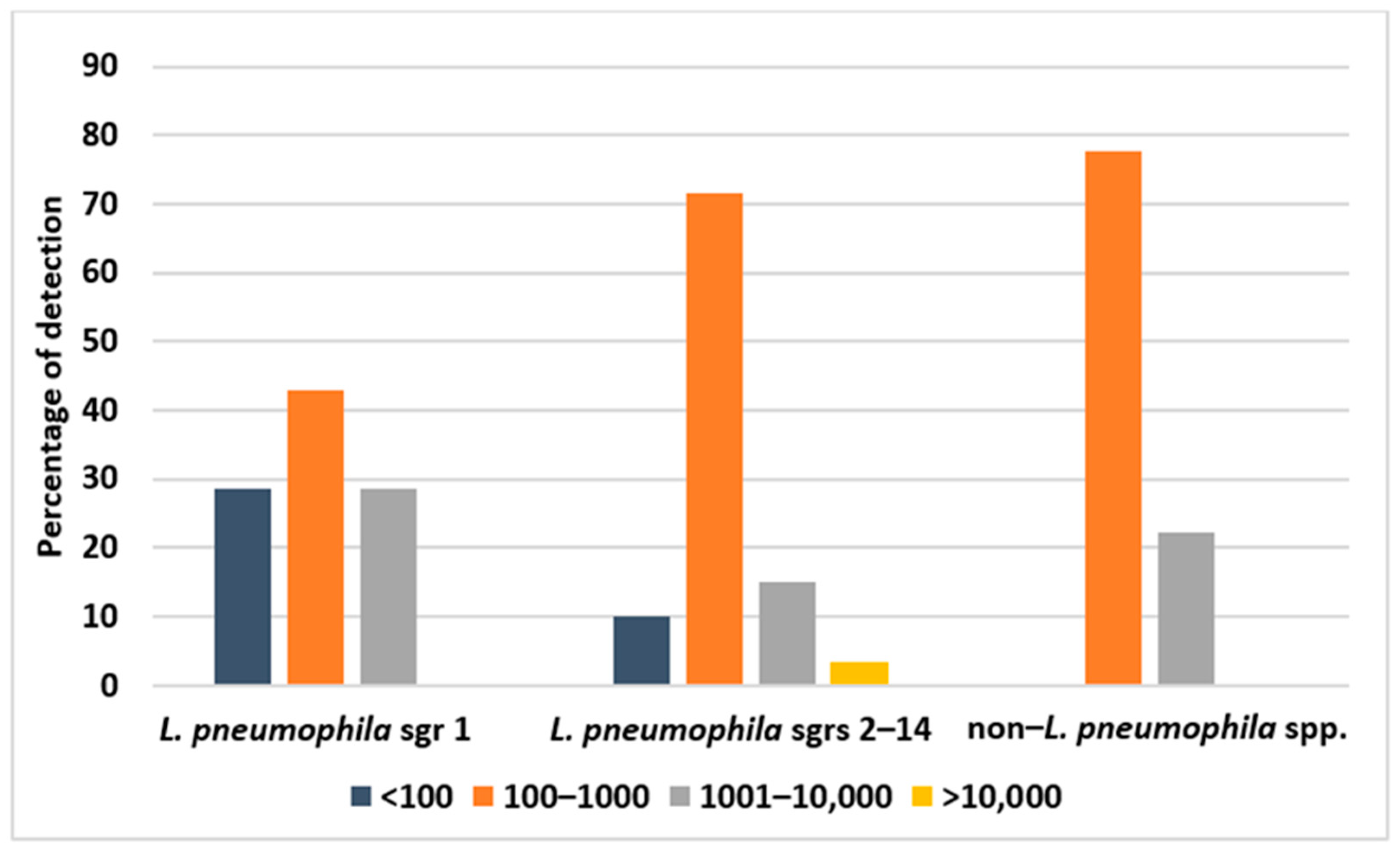
Finally, Table 3 shows the percentages of the Legionella species and serogroups detection in the different typologies of collected samples, while Figure 3 shows the found bacterial loads.
From the table and figure, it is clear that L. pneumophila sgrs 2–14 was by far the most frequently detected bacteria, found especially in swabs and municipal water samples. For the most part, these bacteria were detected with intermediate loads (100–1000 CFUs/L). Bacteria not belonging to the species L. pneumophila accounted for just under one fifth, for the most part with intermediate loads and, for just over 20%, with high loads (1000–10,000 CFUs/L). L. pneumophila 1 accounted for less than 10% of the detected species but, for almost 30%, it was detected with high loads, higher than 1000 CFUs/L. Moreover, it was detected for the most part in thermal water samples compared to the other samples.
4. Discussion
Thermal facilities represent an important economic resource and a pole of attraction both for well-being and for fun. These facilities are often structures capable of providing health services from which a large number of users/customers take advantage, including “vulnerable” people who that can be at risk of infectious complications (i.e., the elderly, people affected by COPD, immunocompromised people). However, these structures are not always subjected to careful surveillance concerning the presence of Legionella spp. The European Directive 80/777/EEC, from which derives the Italian Legislative Decree n. 105 of 25 January 1992 on the use and marketing of natural mineral waters, explicitly excludes that thermal waters are subjected to the same legislation [40]. To date, Italian legislation does not specify the sampling and microbiological checks to be carried out on mineral waters used for curative purposes by spas. However, as specified by Legislative Decree No. 393 of 4 August 1999, the spring water used by spas cannot be subjected to purification treatments nor to the addition of bactericidal/bacteriostatic substances or to any other treatment able to modify its microbial content [41]. While in the previous 2000 Italian guidelines concerning the prevention and control of legionellosis, it was specified that, since thermal waters cannot be treated, other measures can be implemented (e.g., adequate plant design), avoiding the use of material and of components that can favor the growth of Legionella spp. or the slowing down of the flow water [38], the last 2015 guidelines, at point 3.3, specify that it is possible to perform operations similar to those foreseen on normal sanitary networks, including disinfection with chemical or physical means, trying to safeguard the characteristics of thermal waters [39]. Moreover, the guidelines for managers of tourist accommodation facilities and spas show the risk prevention and control measures for Legionella spp. exposure, recommending a monitoring of the facilities every 6 months, after each period of closure of the structure and before the restart of activities, with the indication of remediation interventions in case of bacterial loads >100 CFUs/L [42]. These aspects highlight the complexity of the issue. Indeed, if on one hand it is necessary to maintain the naturalness of the water, on the other hand, is equally important to guarantee its healthiness.
Recently, the Italian Higher Health Institute (ISS), issued some documents containing specific recommendations about the prevention, control, and management of Legionella risk in different water systems in the light of the COVID-19 emergency. In particular, these documents involved all the tourist-accommodation facilities and the dental units. Indeed, due to the lockdown characterizing this period, the occasional use and the possible stagnation of water could represent a serious risk for the transmission of the disease [43,44].
Following to these considerations, it appears extremely important to monitor, over time, the health of the water supplied and the risk of legionellosis transmission represented by these methods. In Europe and in Italy, the number of reported cases of legionellosis has increased steadily over the years, even due to the numerous receptive structures (hotels, spas, etc.) present in the territory [45]. Very little is known about the actual role played by the thermal/mineral springs facilities.
A recent systematic review [46] included the most significant research papers focused on this topic. The analysis covered a very long period (1980–2015) and showed that in this period, the reported events of legionellosis from recreational water involved 10 countries, with the highest number of events (18) and cases (385) in Japan, where attending hot spring spas and public baths is a long tradition and a very widespread habit and water temperature is higher than that used in Europe [47]. The paper included events of both Pontiac fever and legionnaires’ disease occurred in different water settings, among which nine outbreaks (56.2% of all the events) of legionnaires’ disease were reported from hot springs/thermal spas. In these contexts, environmental analysis showed the presence of different serogroups of L. pneumophila (1,2,3,6,9,13) and other species (L. dumoffii, L. londiniensis) at very high load (from 1,600,000 to 15,000,000 CFU/L).
In our study, of 409 collected samples, the percentage of those positive to Legionella spp. was 17.1%, a relative low rate considering the total number of samples and the long period of surveillance. The majority of positive samples were swabs rubbed on taps, showers, and bathtubs of some therapy rooms (mud therapy and inhalation), municipal water samples, and, to a lesser extent, thermal water samples. For these kinds of samples, tanks in particular were the principal sources of Legionella spp. Concerning the species, the majority of those detected were L. pneumophila sgrs 2–14, while L. pneumophila sgr 1 accounted only for less than 10%. However, the recorded bacterial load was rather low, in the majority of cases not exceeding the 1000 CFUs/L. Only in a small percentage and for all three searched Legionella types, the load was >1000. Moreover, the positivity trend had a non-linear tendency, with peaks and valleys, probably due to the measures that were put in place following our reports, and, in any case, there were a general tendency to the decrease in the rate of positivity over time. In addition, we found an important and statistically significant difference between the first 8 years of surveillance and the second ones. Therefore, we can probably assume that an increase in knowledge and awareness of risks associated with recreational water occurred in recent years, leading to an improvement in the management and control measures of this kind of setting. This assumption could have different explanations, among which our constant surveillance over time could have played an important role in increasing this awareness. Moreover, this finding could also be explained by the issuing, in 2006, of the WHO international guidelines on the control of legionellosis in recreational facilities recommending the implementation of safety plans and adequate control measures in pools and hot tubs [48]. These findings show the great importance of a continuous surveillance system.
An important difference was found, finally, between the positivity rate of samples collected in therapies rooms and samples collected in other sources (water storages and customers’ rooms). We assume that this is a critical point to emphasize, given that in therapeutic activities, a concrete risk of becoming infected is present, especially for some activities such as insufflations and aerosol therapy in which a direct entry of pathogens in the airways can occur. However, the reduction in the positivity rate found during the surveillance concerned all the settings and environments of the studied facilities.
The limited number of water samples which showed a critical concentration of Legionella spp. show the effectiveness of control measures adopted in these kinds of facilities, in line with the relative Italian guidelines [49]. Control measures are effective to generally maintain contamination rates below 103 CFUs/L, values that are not indicative of a real infective risk in exposed people. It is important to emphasize the very low presence or the absence of Legionella in vapors and air/gas mixtures used for inhalation. This finding could be explained by the particular chemical composition of the water used in such therapies, which rich in sulfurs [10].
Therefore, our data showed that in the analyzed thermal/mineral springs facilities, the Legionella colonization of the various sites and the subsequent risk for customers to contract legionellosis is rather restrained. Nevertheless, the increasingly frequent use of this type of care and the peculiarity of the customers that often suffer from chronic disease promoting the risk to contract infections require a continuous and targeted surveillance.
A mention must be made regarding the COVID-19 pandemic and its impact on the environment [50], human health, society, and habits [51]. Following this exceptional situation that has modified many different aspects of human life, especially those linked to recreational activities, thermal facilities remained close for a quite long period of time. This situation caused all surveillance activities to cease. Currently, with the partial reduction in the pandemic and the improvement of health conditions, these structures have restarted their activity. This could be a risk because it is well known how the lack of use of water causes water stagnation inside pipelines, which is one of the most critical factors favoring the growth of Legionella spp. This aspect requires a deep and careful evaluation of the risk.
5. Conclusions
A significant increase in visiting thermal facilities and spas both for health and recreational purposes occurred in recent times for many reasons. However, these facilities can represent a risk for contracting legionellosis due to all the activities using water that occur inside them. For this reason, a continuous surveillance with the evaluation of Legionella spp. presence in pipelines is an essential step in order to reduce water contamination and risk for customers. Moreover, other control measures such as disinfection or thermal shock should be performed, even in the presence of low levels of contamination. Actions against biofilm formation is also essential and, in this view, the use of innovative systems could be very helpful [52]. Finally, more and more improvement of laboratory detection could make the difference as much as innovative and effective treatments [53]. This is important not only for healthcare settings, where people are more susceptible to contract infections, but also for thermal facilities that provide therapies and recreational activities to people often with more or less critical health conditions.
Author Contributions
Conceptualization, P.L.; methodology, A.F. and P.L.; formal analysis, M.E.G.; writing—original draft preparation, A.F. and P.L.; resources, M.E.G.; Supervision, S.A.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
All data in this study have been included in the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rota, M.C.; Caporali, M.G.; Bella, A.; Scaturro, M.; Giannitelli, S.; Ricci, M.L. I risultati del sistema di sorveglianza della legionellosi in Italia nel 2020 durante la pandemia di COVID-19. Boll. Epidemiol. Naz. 2021, 2, 9–16. [Google Scholar]
- Laganà, P.; Caruso, G.; Piccione, D.; Gioffrè, M.E.; Pino, R.; Delia, S. Legionella spp., amoebae and not-fermenting Gram negative bacteria in an Italian university hospital water system. Ann. Agric. Environ. Med. 2014, 21, 489–493. [Google Scholar] [PubMed]
- Laganà, P.; Moscato, U.; Poscia, A.; La Milia, D.I.; Boccia, S.; Avventuroso, E.; Delia, S. Geostatistics—A tool applied to the distribution of Legionella pneumophila in a hospital water system. Ann. Agric. Environ. Med. 2015, 22, 655–660. [Google Scholar] [CrossRef] [PubMed]
- Laganà, P.; Delia, S.; Avventuroso, E.; Casale, M.; Dattilo, G. Risk assessment of legionellosis in cardiology units. J. Prev. Med. Hyg. 2017, 58, E173–E176. [Google Scholar]
- Laganà, P.; Gambuzza, M.E.; Delia, S. Legionella risk assessment in cruise ships and ferries. Ann. Agric. Environ. Med. 2017, 24, 276–282. [Google Scholar]
- Laganà, P.; Facciolà, A.; Palermo, R.; Delia, S. Environmental Surveillance of Legionellosis within an Italian University Hospital-Results of 15 Years of Analysis. Int. J. Environ. Res. Public Health 2019, 16, 1103. [Google Scholar]
- Stilo, A.; Troiano, G.; Melcarne, L.; Gioffrè, M.E.; Nante, N.; Messina, G.; Laganà, P. Hand washing in operating room: A procedural comparison. Epidemiol. Biostat. Public Health 2016, 13, e11734-1–e11734-7. [Google Scholar]
- Montagna, M.T.; Cristina, M.L.; De Giglio, O.; Spagnolo, A.M.; Napoli, C.; Cannova, L.; Deriu, M.G.; Delia, S.A.; Giuliano, A.; Guida, M.; et al. Serological and molecular identification of Legionella spp. isolated from water and surrounding air samples in Italian healthcare facilities. Environ. Res. 2016, 146, 47–50. [Google Scholar] [CrossRef]
- Montagna, M.T.; De Giglio, O.; Cristina, M.L.; Napoli, C.; Pacifico, C.; Agodi, A.; Baldovin, T.; Casini, B.; Coniglio, M.A.; D’Errico, M.M.; et al. Evaluation of Legionella Air Contamination in Healthcare Facilities by Different Sampling Methods: An Italian Multicenter Study. Int. J. Environ. Res. Public Health 2017, 14, 670. [Google Scholar] [CrossRef]
- Borella, P.; Montagna, M.T.; Stampi, S.; Stancanelli, G.; Romano Spica, V.; Triassi, M.; Marchesi, I.; Bargellini, A.; Tato, D.; Napoli, C.; et al. Legionella contamination in hot water of Italian hotels. Appl. Environ. Microbiol. 2005, 71, 5805–5813. [Google Scholar]
- Leoni, E.; De Luca, G.; Legnani, P.; Sacchetti, R.; Stampi, S.; Zanetti, F. Legionella waterline colonization: Detection of Legionella species in domestic, hotel and hospital hot water systems. J. Appl. Microbiol. 2005, 98, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Delia, S.; Laganà, P.; Minutoli, E.; Cannavò, G.; Parisi, S. Prevention of legionellosis in hotel establishments: A proposal to introduce a plan of action in accordance with Provision 13 January 2005 (Italy). Ig. Sanita Pubblica 2008, 64, 485–507. [Google Scholar]
- Montagna, M.T.; De Giglio, O.; Napoli, C.; Cannova, L.; Cristina, M.L.; Deriu, M.G.; Delia, S.A.; Giuliano, A.; Guida, M.; Laganà, P.; et al. Legionella spp. contamination in indoor air: Preliminary results of an Italian multicenter study. Epidemiol. Prev. 2014, 38, 62–65. [Google Scholar]
- Sciuto, E.L.; Laganà, P.; Filice, S.; Scalese, S.; Libertino, S.; Corso, D.; Faro, G.; Coniglio, M.A. Environmental management of Legionella in domestic water systems: Consolidated and innovative approaches for disinfection methods and risk assessment. Microorganisms 2021, 9, 577. [Google Scholar] [CrossRef]
- Walser, S.M.; Gerstner, D.G.; Brenner, B.; Höller, C.; Liebl, B.; Herr, C.E. Assessing the environmental health relevance of cooling towers—A systematic review of legionellosis outbreaks. Int. J. Hyg. Environ. Health 2014, 217, 145–154. [Google Scholar]
- Pasquarella, C.; Veronesi, L.; Napoli, C.; Castiglia, P.; Liguori, G.; Rizzetto, R.; Torre, I.; Righi, E.; Farruggia, P.; Tesauro, M. Microbial environmental contamination in Italian dental clinics: A multicenter study yielding recommendations for standardized sampling methods and threshold values. Sci. Total Environ. 2012, 420, 289–299. [Google Scholar] [PubMed]
- Ricci, M.L.; Fontana, S.; Pinci, F.; Fiumana, E.; Pedna, M.F.; Farolfi, P.; Sabattini, M.A.; Scaturro, M. Pneumonia associated with a dental unit waterline. Lancet 2012, 379, 684. [Google Scholar]
- Dallolio, L.; Scuderi, A.; Rini, M.S.; Valente, S.; Farruggia, P.; Bucci Sabattini, M.A.; Pasquinelli, G.; Acacci, A.; Roncarati, G.; Leoni, E. Effect of different disinfection protocols on microbial and biofilm contamination of dental unit waterlines in community dental practices. Int. J. Environ. Res. Public Health 2014, 11, 2064–2076. [Google Scholar]
- Leoni, E.; Dallolio, L.; Sanna, T.; Stagni, F.; D’Alessandro, G.; Piana, G. Impact of a risk management plan on Legionella contamination of dental unit water. Int. J. Environ. Res. Public Health 2015, 12, 2344–2358. [Google Scholar]
- Tuvo, B.; Totaro, M.; Cristina, M.L.; Spagnolo, A.M.; Di Cave, D.; Profeti, S.; Baggiani, A.; Privitera, G.; Casini, B. Prevention and Control of Legionella and Pseudomonas spp. Colonization in Dental Units. Pathogens 2020, 9, 305. [Google Scholar] [CrossRef]
- World Health Organization (WHO). One Health. 2017. Available online: https://www.who.int/news-room/q-a-detail/one-health (accessed on 5 December 2022).
- Van Kenhove, E.; Dinne, K.; Janssens, A.; Laverge, J. Overview and comparison of Legionella regulations worldwide. Am. J. Infect. Control 2019, 47, 968–978. [Google Scholar] [PubMed]
- European Center for Disease Control and Prevention (ECDC). Legionnaires’ Disease—Annual Epidemiological Report for 2020. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/leggionnaires-disease-annual-epidemiological-report-2020.pdf (accessed on 12 December 2022).
- Cunha, B.A.; Cunha, C.B. Legionnaire’s Disease and its mimics: A clinical perspective. Infect. Dis. Clin. 2017, 31, 95–109. [Google Scholar]
- Hamilton, K.A.; Prussin, A.J.; Ahmed, W.; Haas, C.N. Outbreaks of Legionnaires’ Disease and Pontiac Fever 2006–2017. Curr. Environ. Health Rep. 2018, 5, 263–271. [Google Scholar]
- Fraioli, A.; Grassi, M. Medicina Termale, in Strumenti di Medicina Interna-Terapia Medica; Negri, M., Ed.; UTET: Torino, Italy, 2011; pp. 73–84. [Google Scholar]
- Fraioli, A.; Mennuni, G.; Fontana, M.; Nocchi, S.; Ceccarelli, F.; Perricone, C.; Serio, A. Efficacy of Spa Therapy, Mud-Pack Therapy, Balneotherapy, and Mud-Bath Therapy in the Management of Knee Osteoarthritis. A Systematic Review. BioMed Res. Int. 2018, 2018, 1042576. [Google Scholar] [PubMed]
- Ciani, O.; Pascarelli, N.A.; Giannitti, C.; Galeazzi, M.; Meregaglia, M.; Fattore, G.; Fioravanti, A. Mud-Bath Therapy in Addition to Usual Care in Bilateral Knee Osteoarthritis: An Economic Evaluation Alongside a Randomized Controlled Trial. Arthritis Care Res. 2017, 69, 966–972. [Google Scholar]
- Passali, D.; De Corso, E.; Platzgummer, S.; Streitberger, C.; Lo Cunsolo, S.; Nappi, G.; Passali, G.C.; Bellussi, L. Spa therapy of upper respiratory tract inflammations. Eur. Arch. Oto-Rhino-Laryngol. 2013, 270, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Passali, D.; Gabelli, G.; Passali, G.C.; Mösges, R.; Bellussi, L.M. Radon-enriched hot spring water therapy for upper and lower respiratory tract inflammation. Otolaryngol. Pol. 2017, 71, 8–13. [Google Scholar]
- Verhagen, A.P.; Bierma-Zeinstra, S.M.; Boers, M.; Cardoso, J.R.; Lambeck, J.; de Bie, R.; de Vet, H.C. Balneotherapy (or spa therapy) for rheumatoid arthritis. Cochrane Database Syst. Rev. 2015, 2015, CD000518. [Google Scholar] [CrossRef]
- Paoloni, M.; Bernetti, A.; Brignoli, O.; Coclite, D.; Fraioli, A.; Masiero, S.; Napoletano, A.; Quirino, N.; Rengo, F.; Ruosi, C.; et al. Appropriateness and efficacy of Spa therapy for musculoskeletal disorders. A Delphi method consensus initiative among experts in Italy. Ann. Dell’istituto Super. Sanità 2017, 53, 70–76. [Google Scholar]
- Global Wellness Economy Monitor. 2018. Available online: https://globalwellnessinstitute.org/wp-content/uploads/2019/02/GWIWellnessEconomyMonitor2018_022019.pdf?inf_contact_key=e87b822367e20e83dc39630608c964b8f651f238aa2edbb9c8b7cff03e0b16a0 (accessed on 12 December 2022).
- TPT Magazine. L’andamento del Settore Termale in Italia e nel Mondo. 2019. Available online: http://www.toscanapromozione.it/magazine/andamento-settore-termale-italia-mondo/ (accessed on 12 December 2022).
- Costa, J.; da Costa, M.S.; Veríssimo, A. Colonization of a therapeutic spa with Legionella spp: A public health issue. Res. Microbiol. 2010, 161, 18–25. [Google Scholar]
- Germinario, C.; Tafuri, S.; Napoli, C.; Martucci, V.; Termite, S.; Pedote, P.; Montagna, M.T.; Quarto, M. An outbreak of pneumonia in a thermal water spa contaminated with Pseudomonas aeruginosa: An epidemiological and environmental concern. Afr. J. Microbiol. Res. 2012, 6, 1978–1984. [Google Scholar] [CrossRef]
- Terme Italiane. Le terme della Regione Sicilia. Available online: http://www.termeitaliane.com/benessere-termale-in-sicilia_18#.XKyun1UzaHs (accessed on 15 December 2022).
- Conferenza Permanente per i Rapporti Tra Lo Stato, le Regioni e le Province Autonome di Trento e Bolzano. Linee Guida per la Prevenzione e il Controllo della Legionellosi. Gazzetta Ufficiale, 2000. pp. 1–35. Available online: http://www.gazzettaufficiale.it/eli/gu/2000/05/05/103/sg/pdf (accessed on 15 December 2022).
- Conferenza Permanente per i Rapporti Tra Lo Stato, le Regioni e le Province Autonome di Trento e Bolzano. Linee Guida per la Prevenzione e il Controllo della Legionellosi. 2015. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2362_allegato.pdf (accessed on 21 November 2022).
- Gazzetta Ufficiale della Repubblica Italiana (GURI), Serie Generale N. 39 del 17 Febbraio 1992. Decreto Legislativo 25 Gennaio 1992, N. 105. Attuazione della Direttiva 80/777/CEE Relativa alla Utilizzazione e alla Commercializzazione delle Acque Minerali Naturali. Available online: https://www.gazzettaufficiale.it (accessed on 5 December 2022).
- Gazzetta Ufficiale della Repubblica Italiana (GURI), Serie Generale N. 231 del 01 Ottobre 1999. Decreto Legislativo 4 Agosto 1999, N. 339. Disciplina Delle Acque di Sorgente e Modificazioni al Decreto Legislativo 25 Gennaio 1992, N. 105, Concernente le Acque Minerali Naturali, in Attuazione della Direttiva 96/70/CE. Available online: https://www.gazzettaufficiale.it/eli/id/1999/10/01/099G0410/sg (accessed on 21 November 2022).
- Delia, S.; Laganà, P.; Minutoli, E. Occurrence of Legionella in beach shower facilities. J. Prev. Med. Hyg. 2007, 48, 114–117. [Google Scholar] [PubMed]
- Istituto Superiore di Sanità. Rapporto (ISS). COVID-19 N. 21/2020—Guida per la Prevenzione della Contaminazione da Legionella Negli Impianti Idrici di Strutture Turistico Recettive e Altri Edifici ad uso Civile e Industriale, non Utilizzati Durante la Pandemia COVID-19. Available online: https://www.epicentro.iss.it/coronavirus/pdf/rapporto-covid-19-21-2020.pdf (accessed on 3 November 2022).
- Istituto Superiore di Sanità. Rapporto (ISS). COVID-19 N. 21/2020—Indicazioni per la Prevenzione del Rischio Legionella Nei riuniti Odontoiatrici Durante la Pandemia da COVID-19. Available online: https://www.epicentro.iss.it/coronavirus/pdf/rapporto-covid-19-27-2020.pdf (accessed on 5 December 2022).
- Europan Centre for Disease Control and Prevention (ECDC). Legionnaires’ Disease Surveillance in Europe, 2014; ECDC: Stockholm, Sweden, 2016; Available online: http://ecdc.europa.eu/en/publications-data/legionnairesdisease-europe-2014 (accessed on 3 November 2022).
- Leoni, E.; Catalani, F.; Marini, S.; Dallolio, L. Legionellosis Associated with Recreational Waters: A Systematic Review of Cases and Outbreaks in Swimming Pools, Spa Pools, and Similar Environments. Int. J. Environ. Res. Public Health 2018, 15, 1612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuroki, T.; Ishihara, T.; Ito, K.; Kura, F. Bathwater-associated cases of legionellosis in Japan, with a special focus on Legionella concentrations in water. Jpn. J. Infect. Dis. 2009, 62, 201–205. [Google Scholar]
- World Health Organization (WHO). Guidelines for Safe Recreational Water Environments. Swimming Pools and Similar Environments; WHO: Geneva, Switzerland, 2006; Volume 2, Available online: http://www.who.int/water_sanitation_health/bathing/srwe2full.pdf (accessed on 21 November 2022).
- Linee Guida Recanti Indicazioni Sulla Legionellosi per i Gestori di Strutture Turistico-Recettive e Termali. Gazzetta Ufficiale della Repubblica Italiana. N. 28 Del 04–02–2005. Available online: http://old.iss.it/binary/iss4/cont/28_02_05.1144152817.pdf (accessed on 5 December 2022).
- Facciolà, A.; Laganà, P.; Caruso, G. The COVID-19 pandemic and its implications on the environment. Environ. Res. 2021, 201, 111648. [Google Scholar]
- Clemente-Suárez, V.J.; Navarro-Jiménez, E.; Moreno-Luna, L.; Saavedra-Serrano, M.C.; Jimenez, M.; Simón, J.A.; Tornero-Aguilera, J.F. The Impact of the COVID-19 Pandemic on Social, Health, and Economy. Sustainability 2021, 13, 6314. [Google Scholar]
- Filice, S.; Sciuto, E.L.; Scalese, S.; Faro, G.; Libertino, S.; Corso, D.; Timpanaro, R.M.; Laganà, P.; Coniglio, M.A. Innovative antibiofilm smart surface against Legionella for water systems. Microorganisms 2022, 10, 870. [Google Scholar]
- De Giglio, O.; Diella, G.; Trerotoli, P.; Consonni, M.; Palermo, R.; Tesauro, M.; Laganà, P.; Serio, G.; Montagna, M.T. Legionella Detection in Water Networks as per ISO 11731:2017: Can Different Filter Pore Sizes and Direct Placement on Culture Media Influence Laboratory Results? Int. J. Environ. Res. Public Health 2020, 17, 2077. [Google Scholar]
Figure 1.
The thermal facilities of the Sicily Region, Italy.

Figure 2.
Annual temporal trend of Legionella spp. positivity detected on the collected samples.

Figure 3.
Percentages of bacterial load (CFUs/L) depending on the different detected species.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Absolute numbers of collected and positive samples with positivity percentage per year of surveillance.
Table 1.
Absolute numbers of collected and positive samples with positivity percentage per year of surveillance.
| Year | Collected Samples | Positive Samples | % |
|---|---|---|---|
| 2004 | 26 | 4 | 15.4 |
| 2005 | 33 | 15 | 45.5 |
| 2006 | 26 | 2 | 7.7 |
| 2007 | 24 | 3 | 12.5 |
| 2008 | 51 | 19 | 37.3 |
| 2009 | 26 | 0 | 0.0 |
| 2010 | 45 | 11 | 24.4 |
| 2011 | 32 | 0 | 0.0 |
| 2012 | 33 | 6 | 18.2 |
| 2013 | 11 | 1 | 9.1 |
| 2014 | 53 | 4 | 7.5 |
| 2015 | 10 | 0 | 0.0 |
| 2016 | 10 | 0 | 0.0 |
| 2017 | 10 | 2 | 20.0 |
| 2018 | 11 | 2 | 18.2 |
| 2019 | 8 | 1 | 12.5 |
| TOT | 409 | 70 | 17.1 |
Table 2.
Absolute numbers and percentage of positivity found in the different sample typology and collection sites.
Table 2.
Absolute numbers and percentage of positivity found in the different sample typology and collection sites.
| SWABS 37 (52.8%) | |
| Showers and bathtubs of mud therapy rooms | 22 (60%) |
| Showers and taps of aerosol and inhalation rooms | 15 (40%) |
| MUNICIPAL WATER SAMPLES 17 (24.3%) | |
| Collection tanks and boilers | 7 (41.2%) |
| Showers and bathtubs of mud therapy rooms | 5 (29.4%) |
| Taps and showers of customers living rooms | 3 (17.6%) |
| Taps of pulmonary ventilation rooms | 2 (11.8%) |
| THERMAL WATERS SAMPLES 13 (18.6%) | |
| Collection tanks | 9 (66.6%) |
| Showers and bathtubs of mud therapy rooms | 2 (16.8%) |
| Taps of pulmonary ventilation rooms | 1 (8.3%) |
| Taps and showers of customers living rooms | 1 (8.3%) |
| VAPOUR SAMPLES 3 (4.3%) | |
| Nebulization equipment | 3 (100%) |
Table 3.
Percentage of the different Legionella serogroups detected in various typologies of collected samples.
Table 3.
Percentage of the different Legionella serogroups detected in various typologies of collected samples.
| L. pneumophila sgr 1 | L. pneumophila sgrs 2–14 | Non-L. pneumophila | |
|---|---|---|---|
| Swabs | 8.1% | 89.2% | 16.2% |
| Municipal water samples | 11.8% | 82.3% | 5.9% |
| Thermal water samples | 15.4% | 69.2% | 15.4% |
| Vapour samples | 0 | 66.6% | 33.3% |
| Average value | 8.8% | 76.8% | 17.7% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Laganà, P.; Gioffrè, M.E.; Delia, S.A.; Facciolà, A. Legionella spp. in Thermal Facilities: A Public Health Issue in the One Health Vision. Water 2023, 15, 689. https://doi.org/10.3390/w15040689
AMA Style
Laganà P, Gioffrè ME, Delia SA, Facciolà A. Legionella spp. in Thermal Facilities: A Public Health Issue in the One Health Vision. Water. 2023; 15(4):689. https://doi.org/10.3390/w15040689
Chicago/Turabian StyleLaganà, Pasqualina, Maria Eufemia Gioffrè, Santi Antonino Delia, and Alessio Facciolà. 2023. "Legionella spp. in Thermal Facilities: A Public Health Issue in the One Health Vision" Water 15, no. 4: 689. https://doi.org/10.3390/w15040689
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.